ORIF – Conventional plating
1. Principles
Anatomical reduction
Anatomical reduction of the articular fracture component and fixation with lag screws (absolute stability) is ideal.
After reduction of the articular fracture component, anatomical reduction of the metaphyseal component must be achieved.
Double plating
In order to avoid varus collapse on the medial side double plating should be considered and if necessary, carried out. In these fracture patterns the placement of the medial plate may be medial rather than posteromedial. This depends of course on the fracture pattern and forces which must be neutralized.
2. Patient preparation
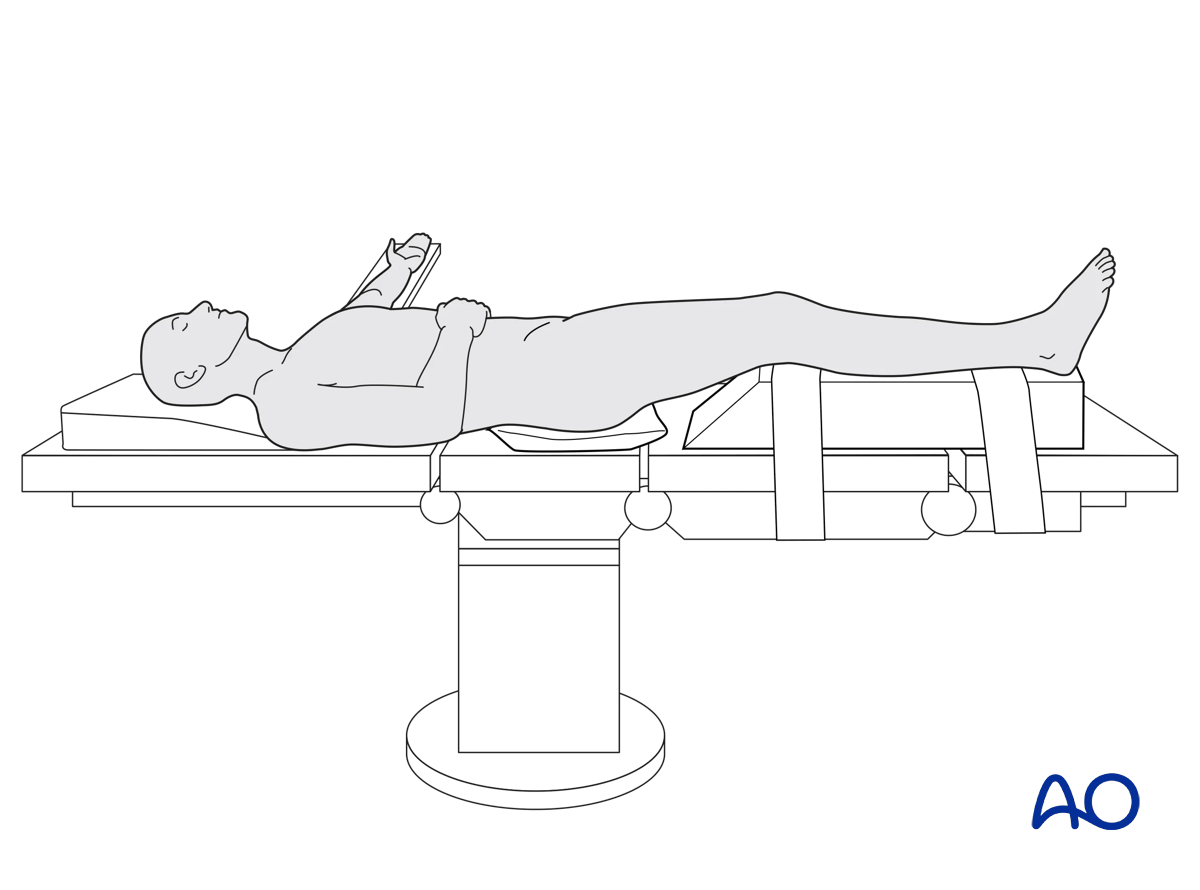
The patient is placed in the Supine position.
3. Approaches
For this procedure the following approaches may be used:
4. Reduction
Open reduction
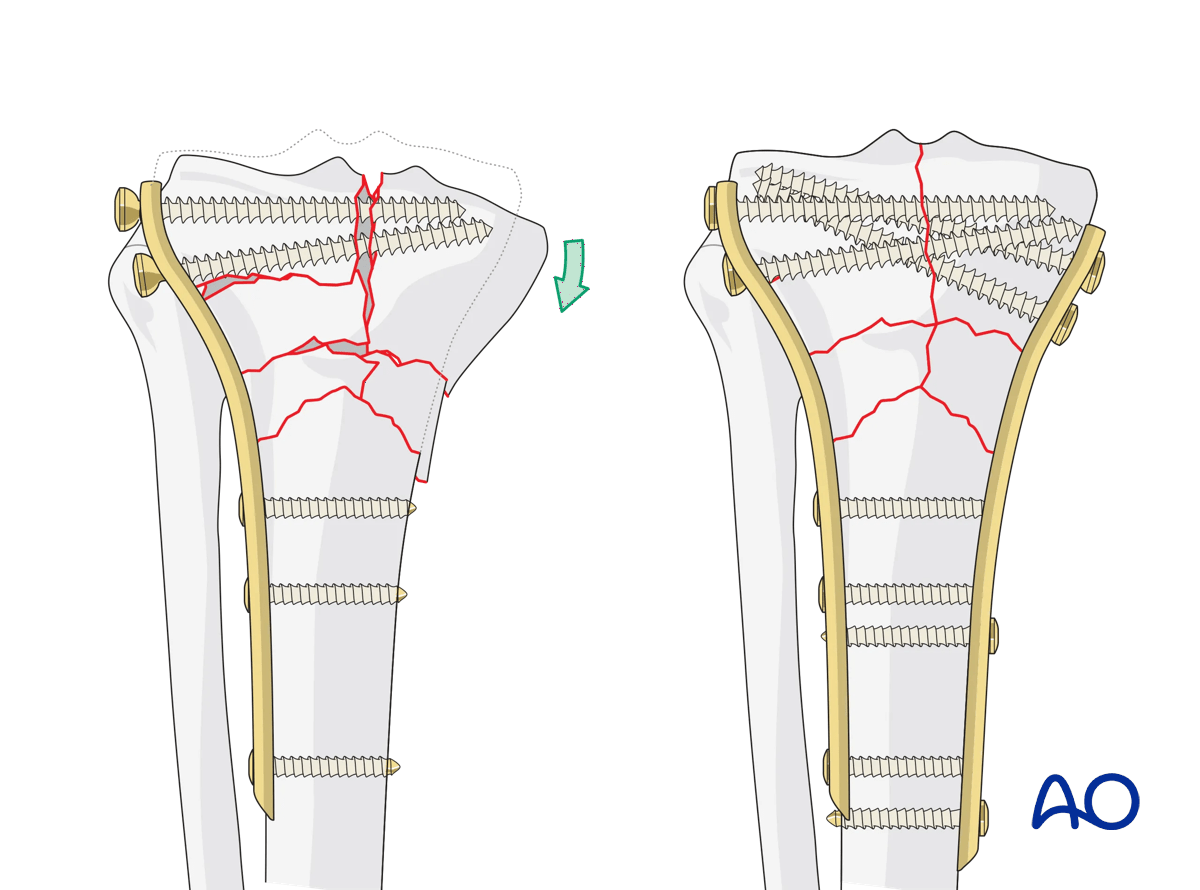
The C2 fracture pattern is best treated with open reduction and direct visualization of the articular surface with indirect reduction of the comminuted metaphysis. The articular reduction can be confirmed under direct visualization or, if not easily visualized, with radiographic confirmation.
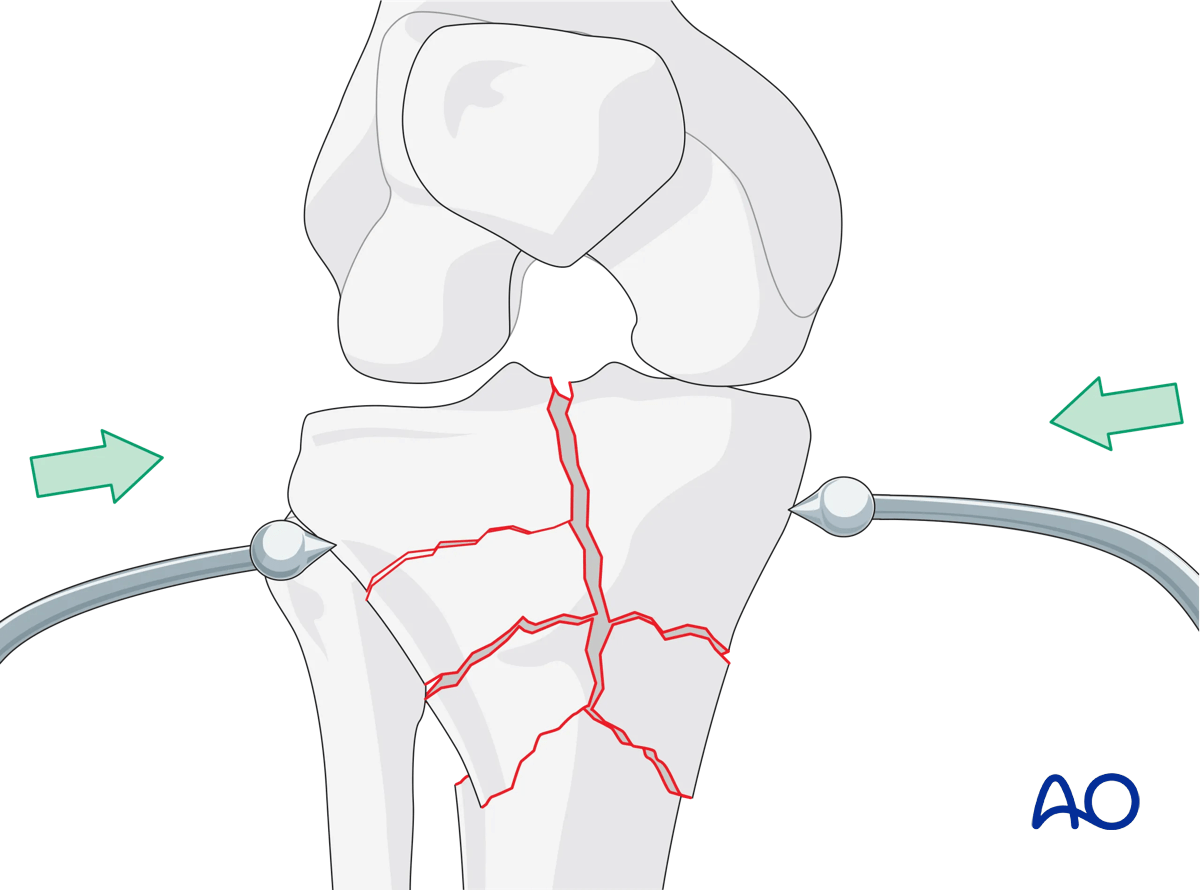
Indirect reduction of the metaphysis may be achieved with external fixation and, if available, anatomically contoured plates.
Given the use of indirect reduction, radiographic confirmation of frontal and sagittal plane alignment is imperative.
Secure reduction
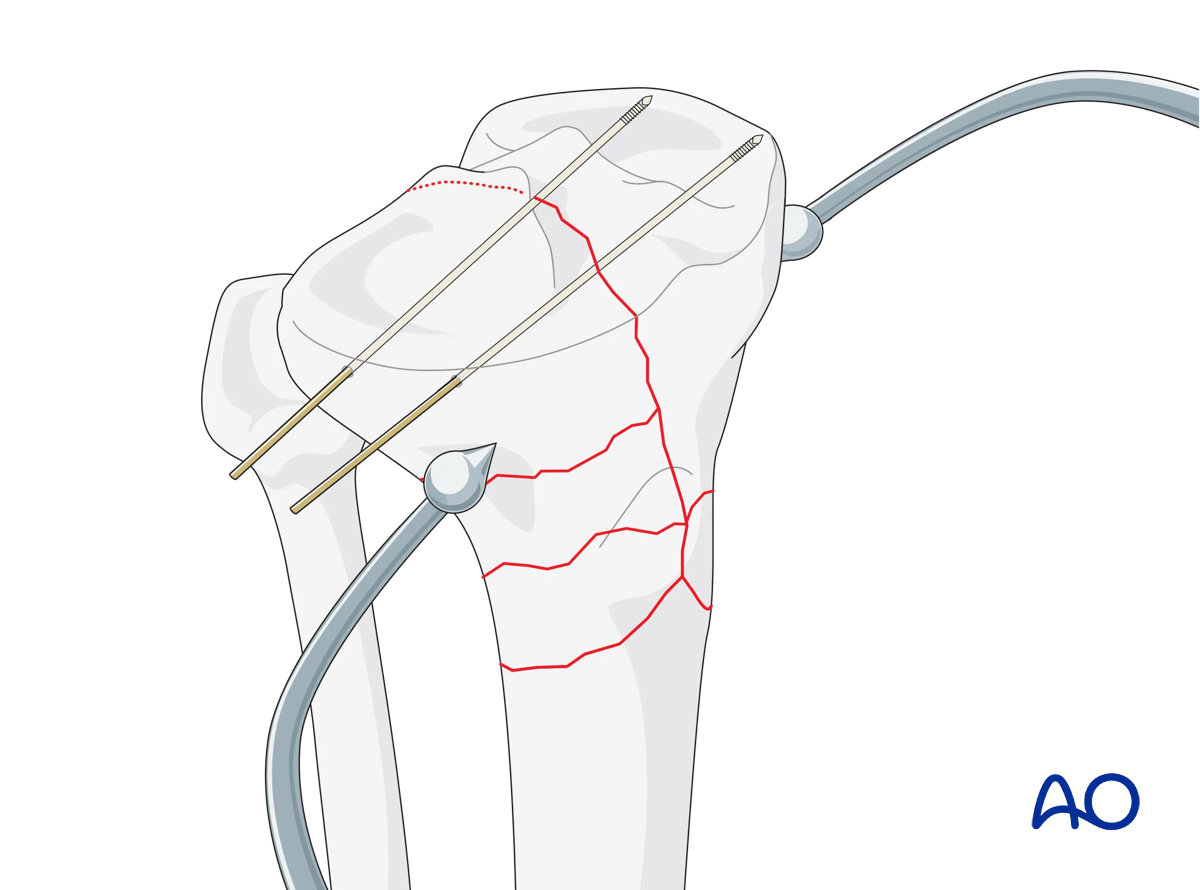
Anatomical reduction of the articular surface is mandatory. Provisional fixation can be performed with K-wires.
In situations where the fracture lines are not directly visualized, positioning of the knee is important for correct reduction and fixation. Frontal and sagittal plane alignment must be confirmed radiographically. The use of an external fixator to directly maintain alignment is extremely helpful.
5. Fixation
Lag screw fixation is preferred across the simple articular reduction. This should ideally be performed through the proximal portion of the lateral plate. The comminuted metaphysis should be stabilized with a relative stability technique on both medial and lateral columns.
Medial column fixation
The medial plate may be applied either posteromedially or medially. The position of the plate is determined by a number of important factors such as the direction of the fracture lines, the forces to be neutralized, the exposure already made, and finally which application will allow for the least traumatic but still biomechanically-sound application.
Lateral column fixation
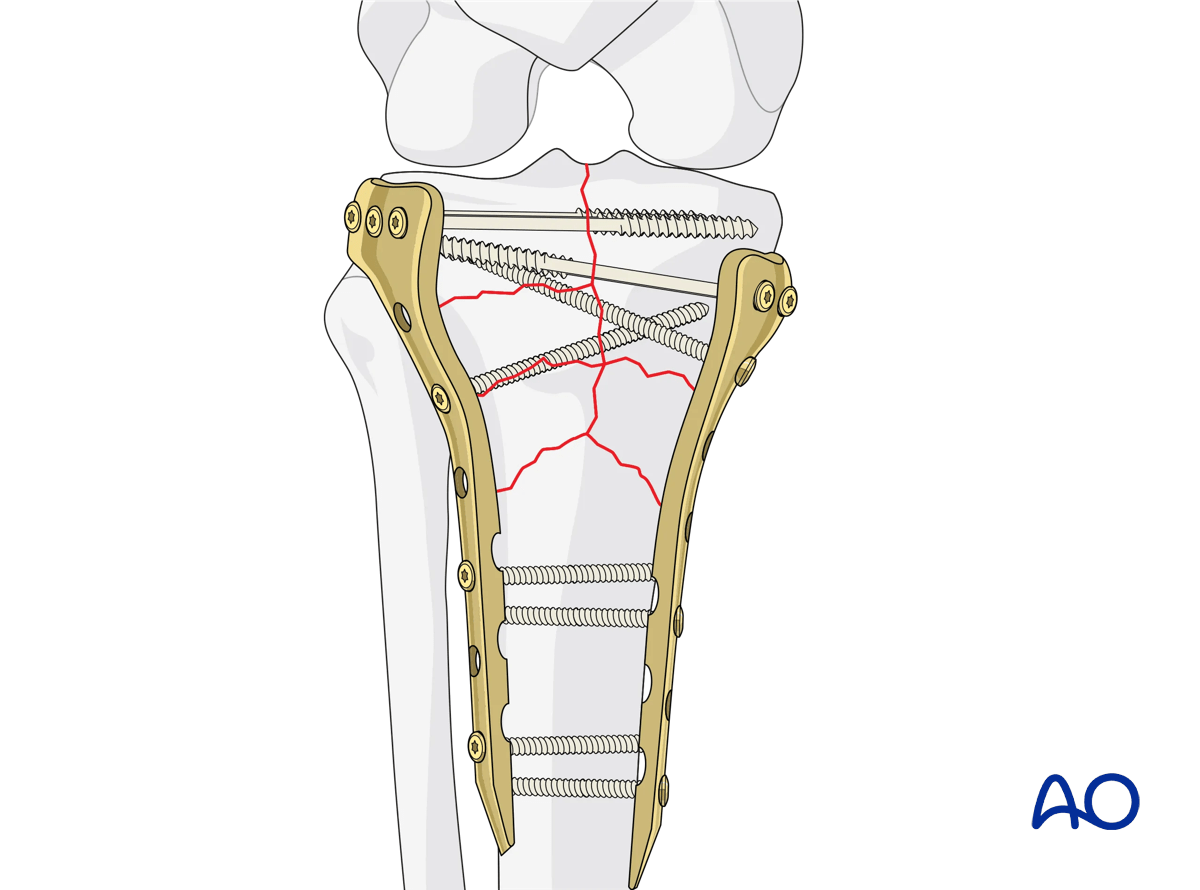
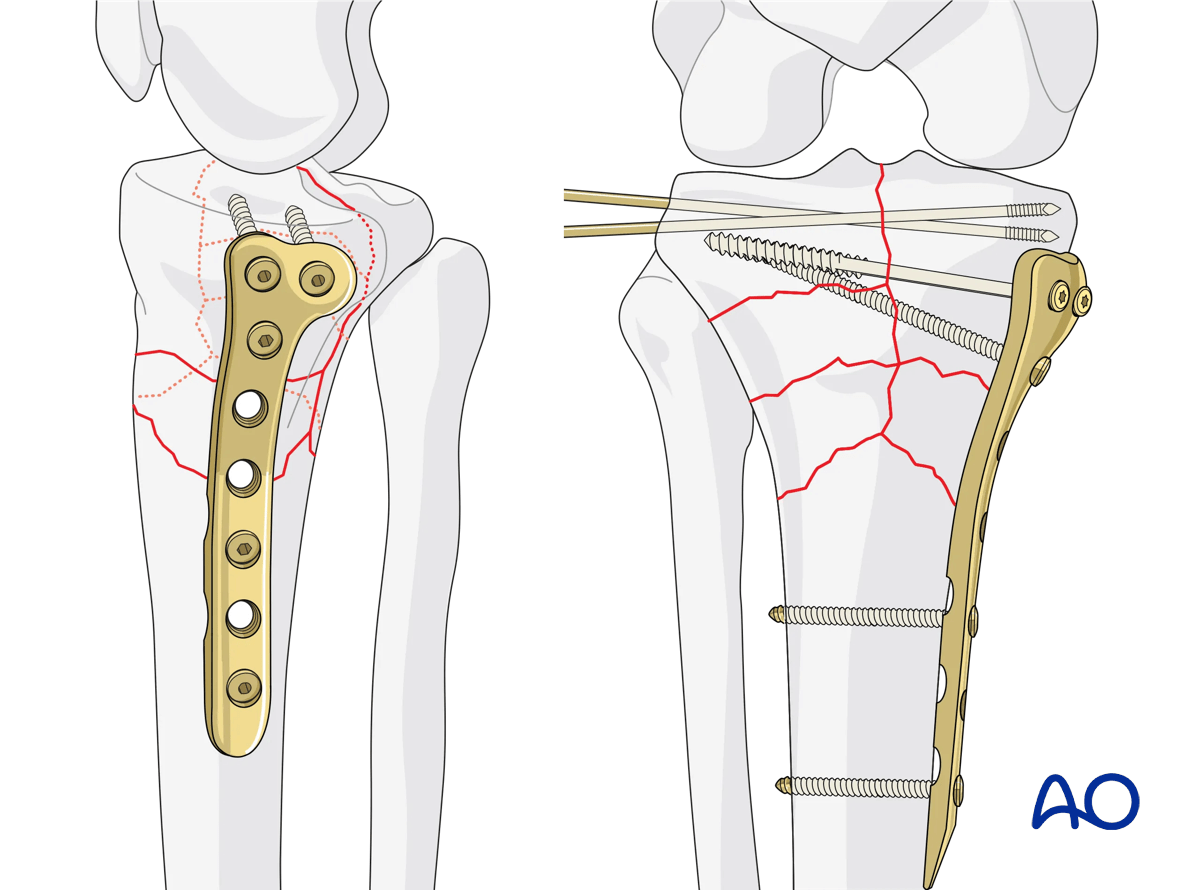
The lateral plate is inserted in the space between muscle and periosteum. The plate must be carefully contoured to the bone. Fixation begins with the insertion of a screw through the plate into the metaphysis, securing the plate to the proximal articular fragment. A second screw should be placed through the distal portion of the plate into the diaphyseal fragment. Fixation is then completed distally. Fixation proximally is then completed with lag screws placed across the articular fracture line. More information on techniques for lag screw insertion can be found in the Basic techniques of fracture management.
The illustration shows the final construct.
6. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













