Medial and posteromedial approach to the proximal tibia
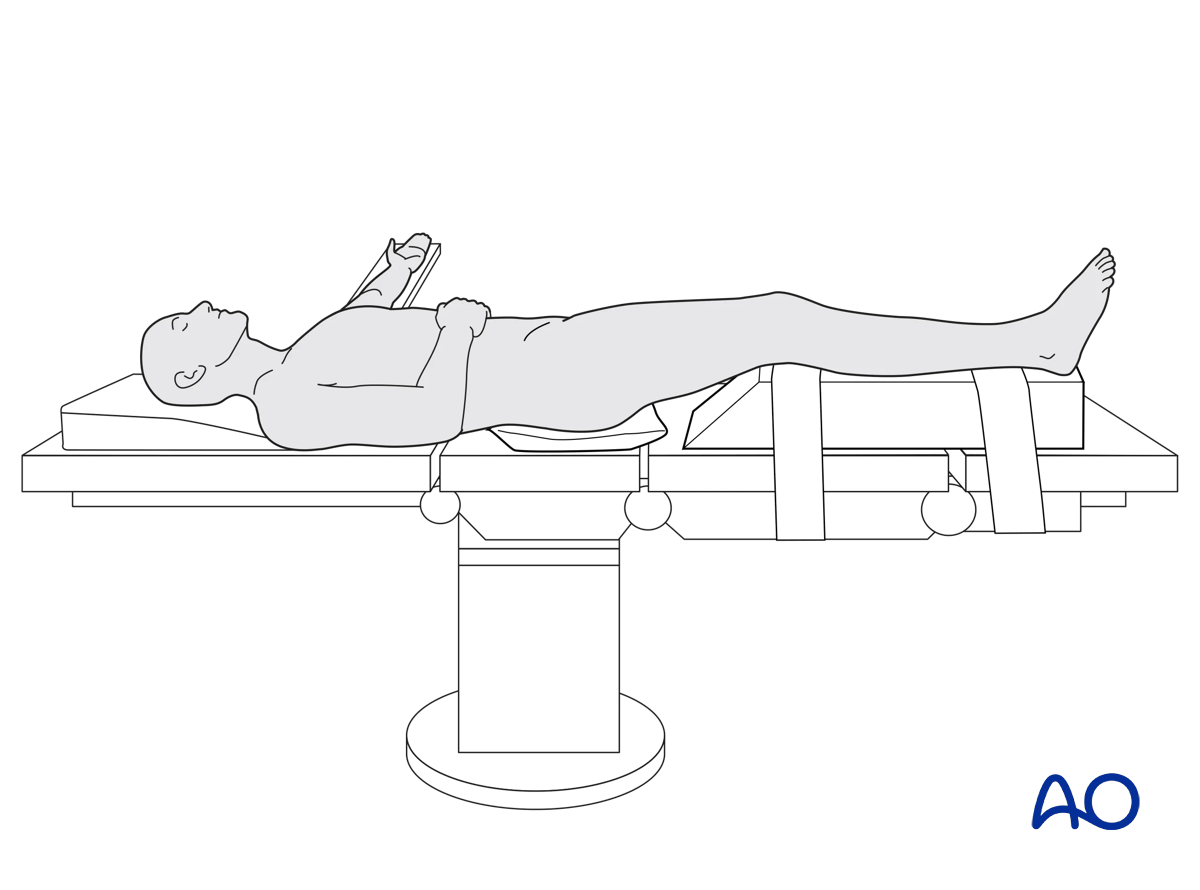
1. Patient positioning
Patients are positioned supine, confirming that full external rotation is not compromised. Ideally, the patella should be pointing directly anterior. The image intensifier is brought in from the ipsilateral injured side.
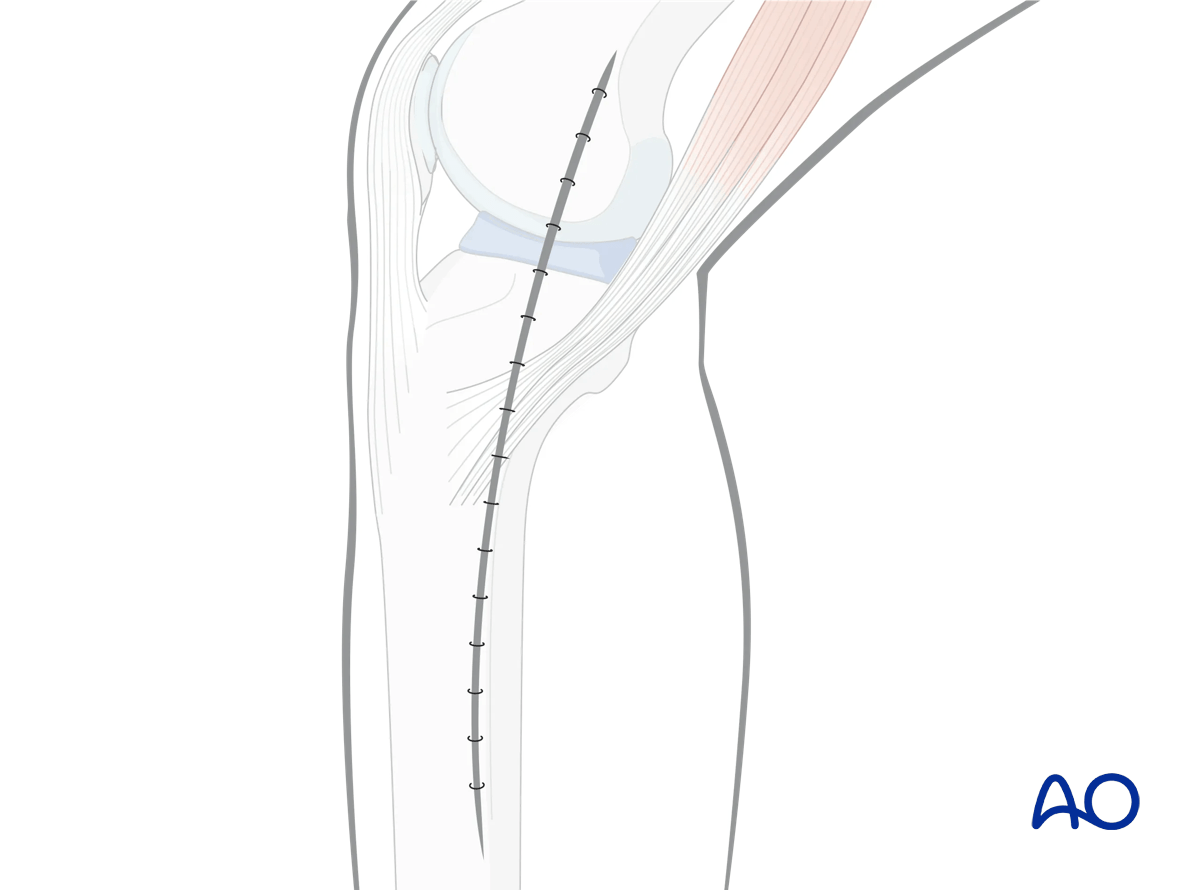
2. Skin incision
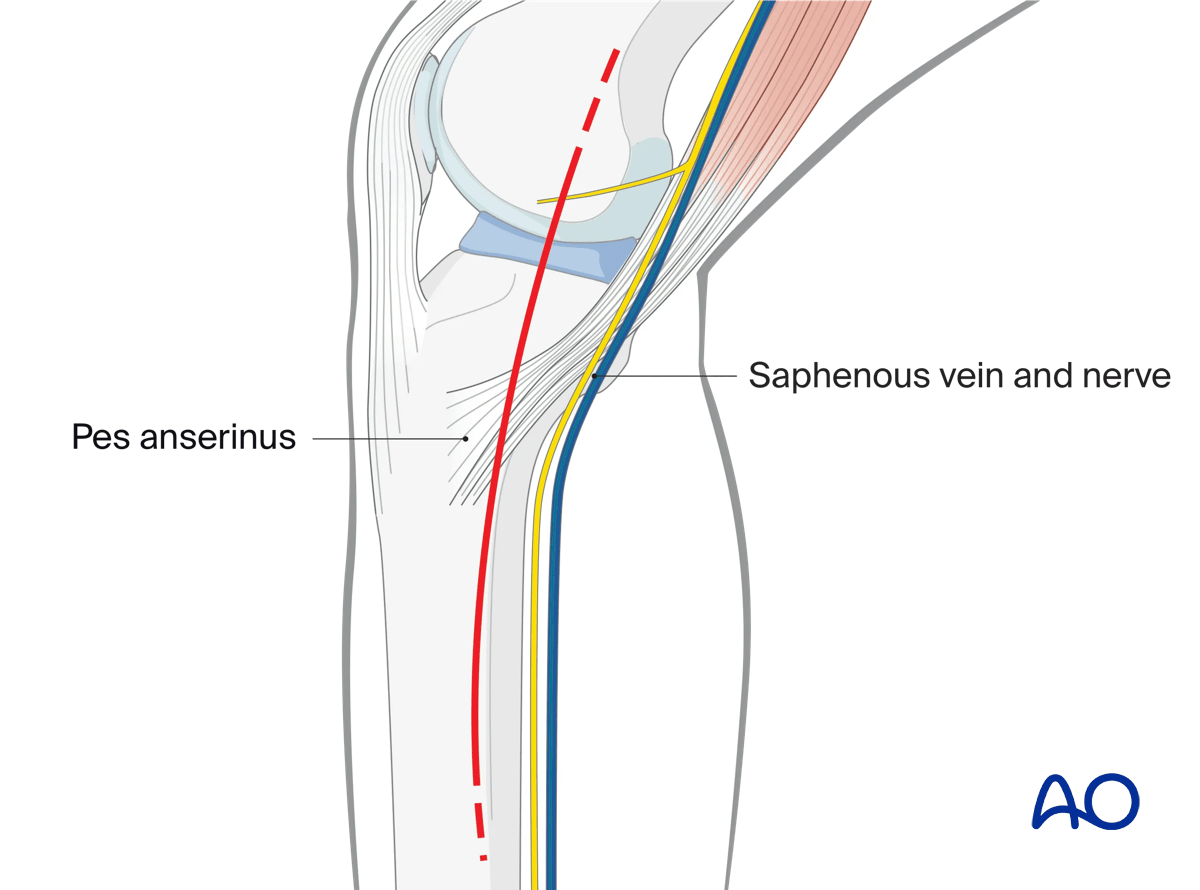
The incision is typically just posterior to the posteromedial crest of the tibia. If more posteromedial work is anticipated, then the skin incision can curve posteriorly, and follow the course of the posterior aspect of the pes anserinus tendons. If anteromedial work is anticipated, the incision can be kept straight.
The superficial dissection should minimize injury to the saphenous vein and nerve.
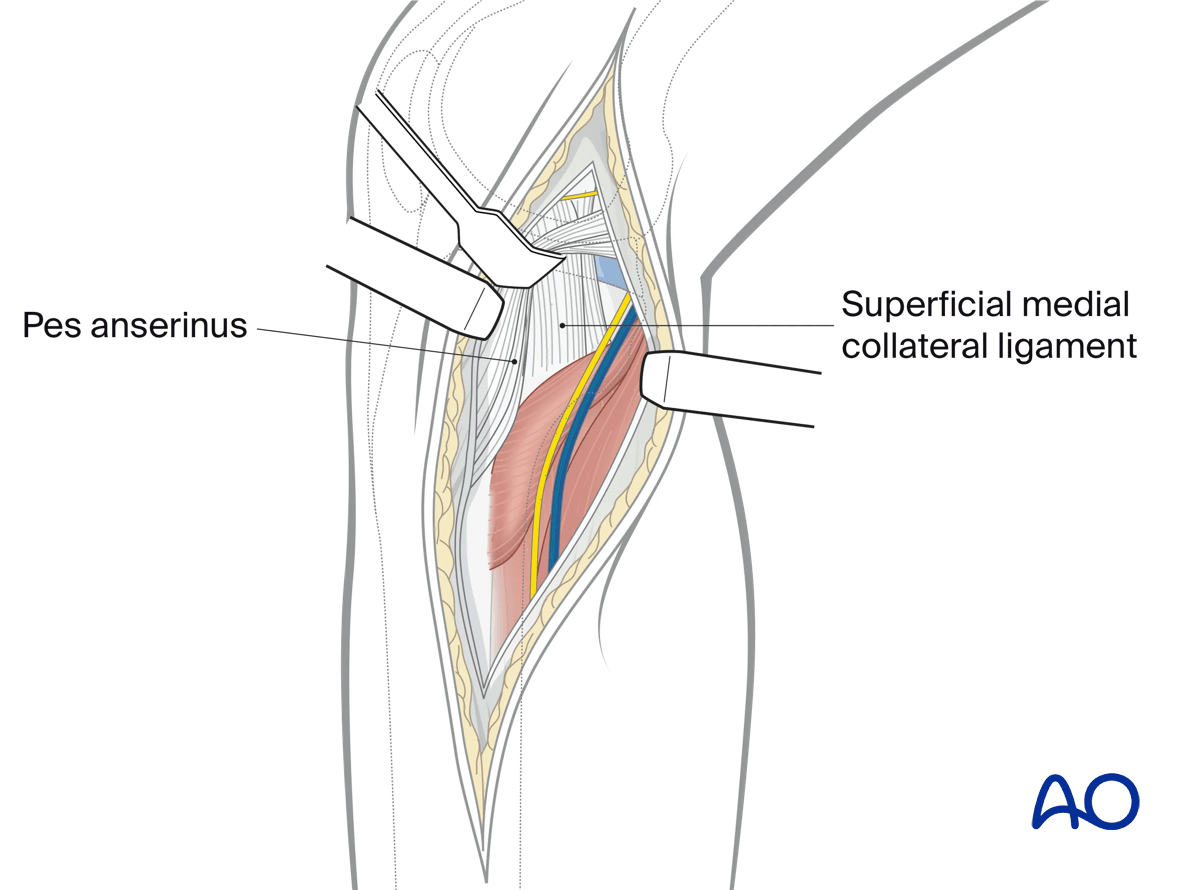
3. Deep dissection
In the distal part of the wound the fascia over the medial head of the gastrocnemius is incised longitudinally. A gloved finger is inserted from distal to proximal under the fascia to identify the pes anserinus tendons. The fascial incision can now proceed proximally and posteriorly, avoiding transection of those tendons. The pes anserinus tendons can now be retracted anteriorly, revealing the underlying superficial medial collateral ligament. Increased mobilization of the pes anserinus tendons is effectively done by transecting the fibrous bands that connect the semitendinosus to the gastrocnemius.
4. Access
Access to the posteromedial plateau
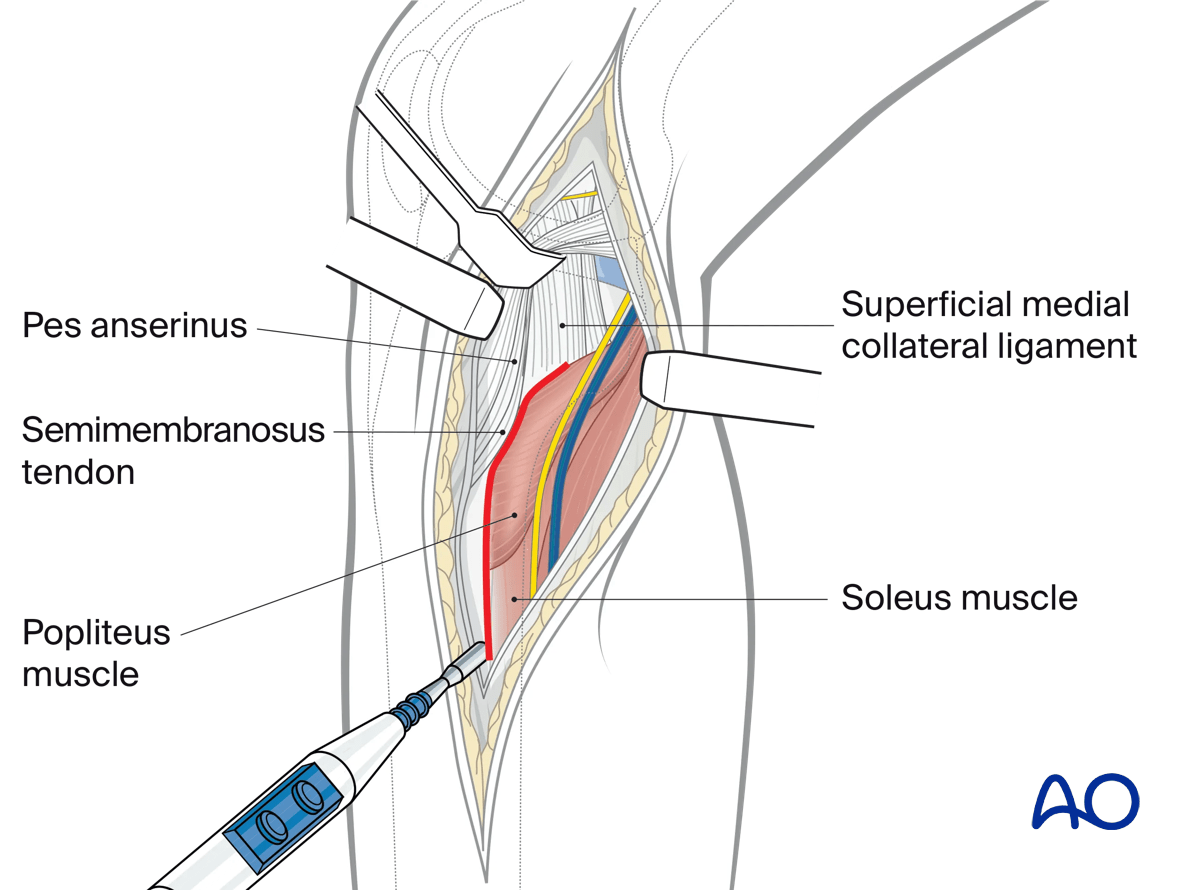
With the pes anserinus tendons retracted anteriorly electrocautery is used to incise the origin of the popliteus muscle proximally and soleus muscle distally from the posteromedial crest of the tibia. This cautery line will follow the posterior aspect of the superficial collateral ligament. Proximally the dissection is limited by the insertion of the semimembranosus tendon.
Subperiosteal dissection of the posteromedial tibial plateau can now be performed. In many instances this will reveal the apex of the posteromedial fracture fragment.
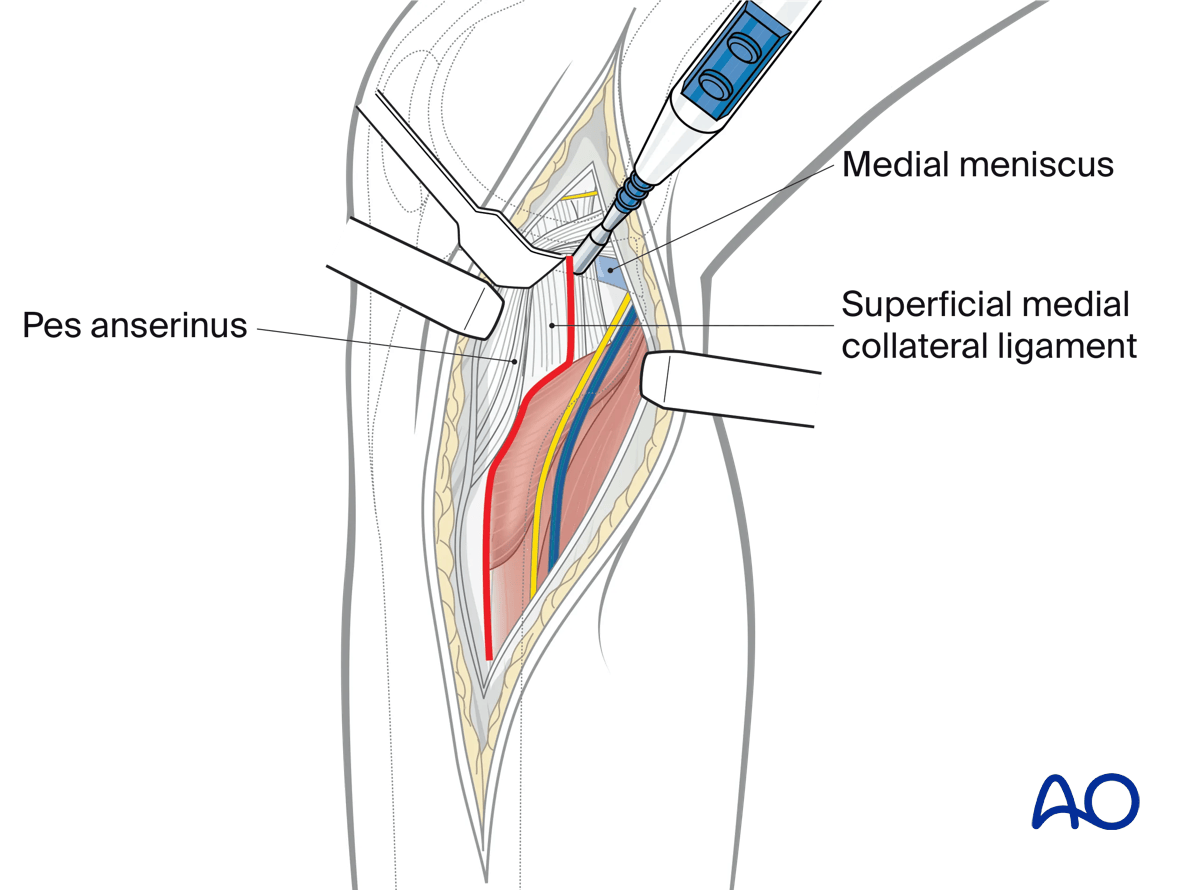
Opening of the knee joint
Visualization of the medial and posteromedial aspect of the medial joint space is not nearly as easy as visualization of the lateral articular surface. This is because the medial collateral ligament is intimately associated with the medial meniscus and the semimembranosus tendon covers the posteromedial tibial plateau.
In patients with a posteromedial articular fracture fragment (coronal plane fracture) the fracture edge is simply followed from distal to proximal until the articular surface is visualized. This often entails exploiting the longitudinal disruption in the superficial medial collateral ligament.
Medial/anteromedial exposure
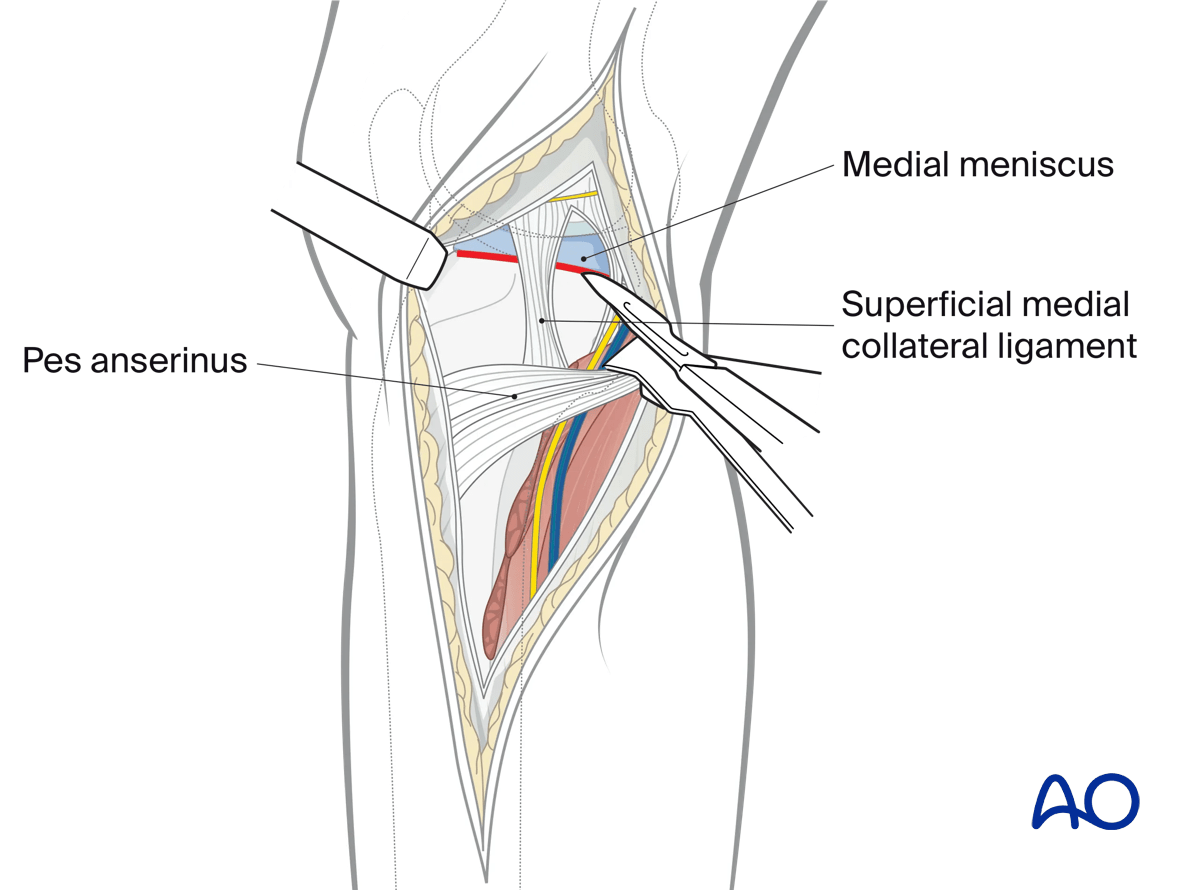
Exposure of the medial/anteromedial part (medial column) of the proximal tibia can be achieved with an anterior subcutaneous dissection. The pes can be retracted posteriorly, first by incising the sartorial fascia just proximal to the gracilis tendon. This will reveal the superficial medial collateral ligament proximal to the pes tendons.
Visualization of the articular surface can now be performed with a submeniscal arthrotomy anterior to the anterior border of the superficial medial collateral ligament.
Pes tendon tenotomy can be performed in situations requiring improved access or visualization of either the posteromedial or anteromedial plateau. A simple repair of the tendons at wound closure can easily be done.
5. Wound closure
Close the capsule. If needed, insert suction drains and close the soft tissues in a routine manner.