Anterolateral and extended anterolateral approach to the proximal tibia
1. Introduction
The anterolateral approach is the most common approach for fractures of the proximal tibia.
This approach is useful for:
- fractures of the lateral column and visualization of the lateral articular surface
- many extraarticular A-type fractures and some simple C-type fracture patterns
The anterolateral approach to the proximal tibia is an extensile approach. Both proximal and distal extensions are possible.
This approach allows visualization of the lateral articular surface, lateral meniscus, and the lateral column of the tibial plateau, as well as access to the anterior tibial tubercle.
Ideal joint visualization requires distraction with the use of a universal distractor or external fixator.
2. Skin incision
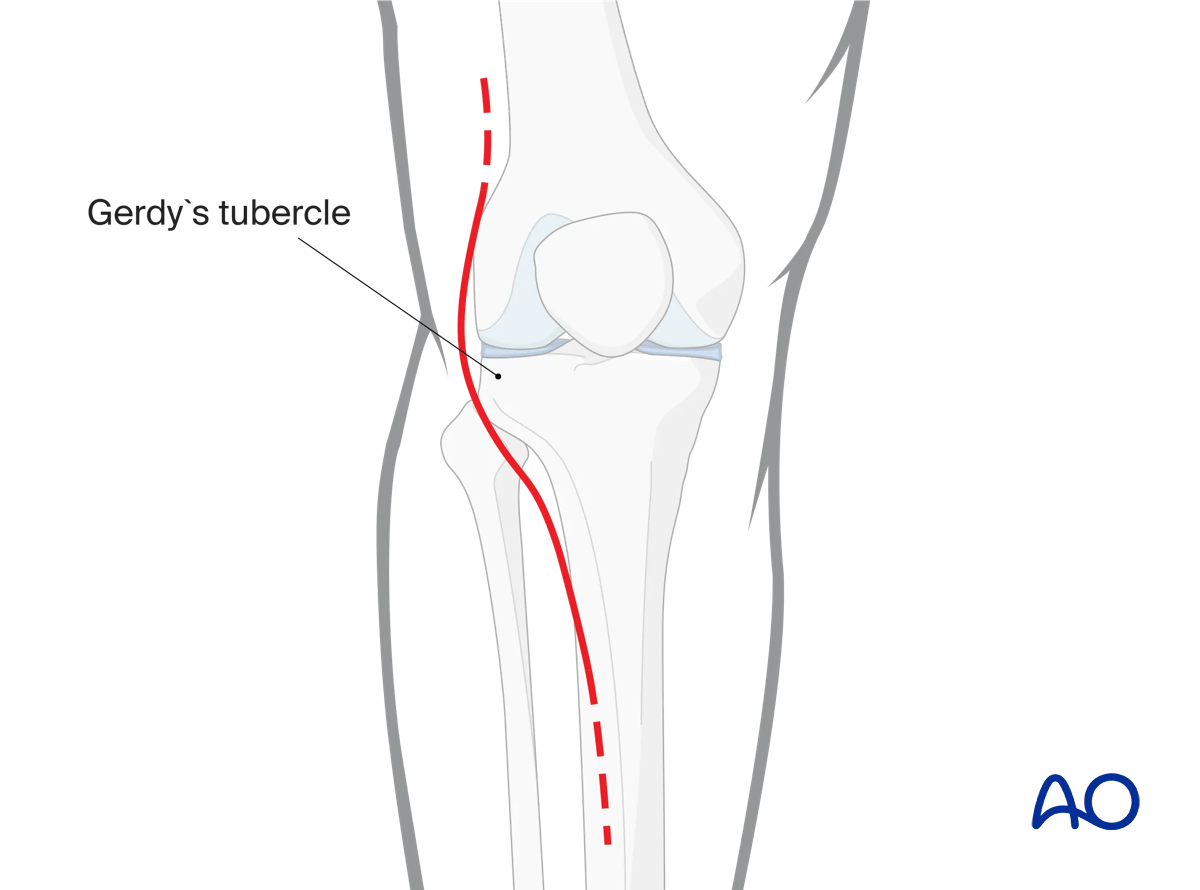
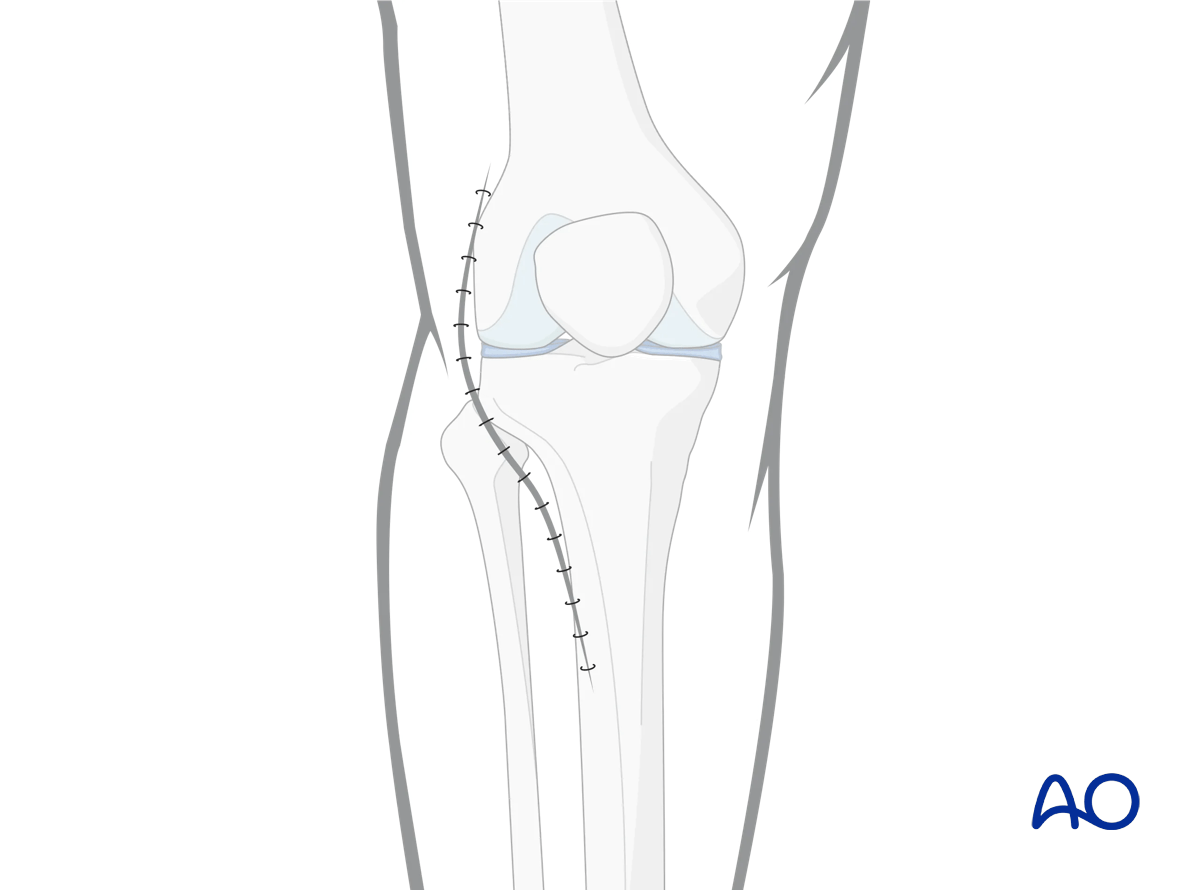
Make a straight incision lateral to the patella.
Incision typically begins in the mid-coronal plane just proximal to the lateral epicondyle of the femur. The incision curves towards Gerdy’s tubercle of the tibia and then proceeds distally in a curvilinear fashion approximately 1cm lateral to the anterior tibial crest.
The distal extent of the incision is dictated by the fracture pattern and anticipated implant length.
The dissection carries through the skin and subcutaneous layer to the underlying fascia.
3. Opening the fascia
Open the deep fascia splitting the ilio-tibial tract to Gerdy’s tubercle.
Beginning proximally, the ilio-tibial band is incised to Gerdy’s tubercle. Care is taken not to incise the underlying joint capsule. The ilio-tibial band is then elevated off its Gerdy’s tubercle insertion both anteriorly and posteriorly. At the distal end of Gerdy’s tubercle the insertion of the ilio-tibial band becomes confluent with the fascia of the anterior compartment. The anterior compartment fascia is incised in continuity with the elevation of ilio-tibial band from Gerdy’s tubercle.
Elevation of the iliotibial band from Gerdy’s tubercle posteriorly is complete once the anterior portion of the fibular head can be identified and palpated through the deep dissection. Anteriorly, elevation of the ilio-tibial band insertion is limited by the lateral fibers of the patella tendon.
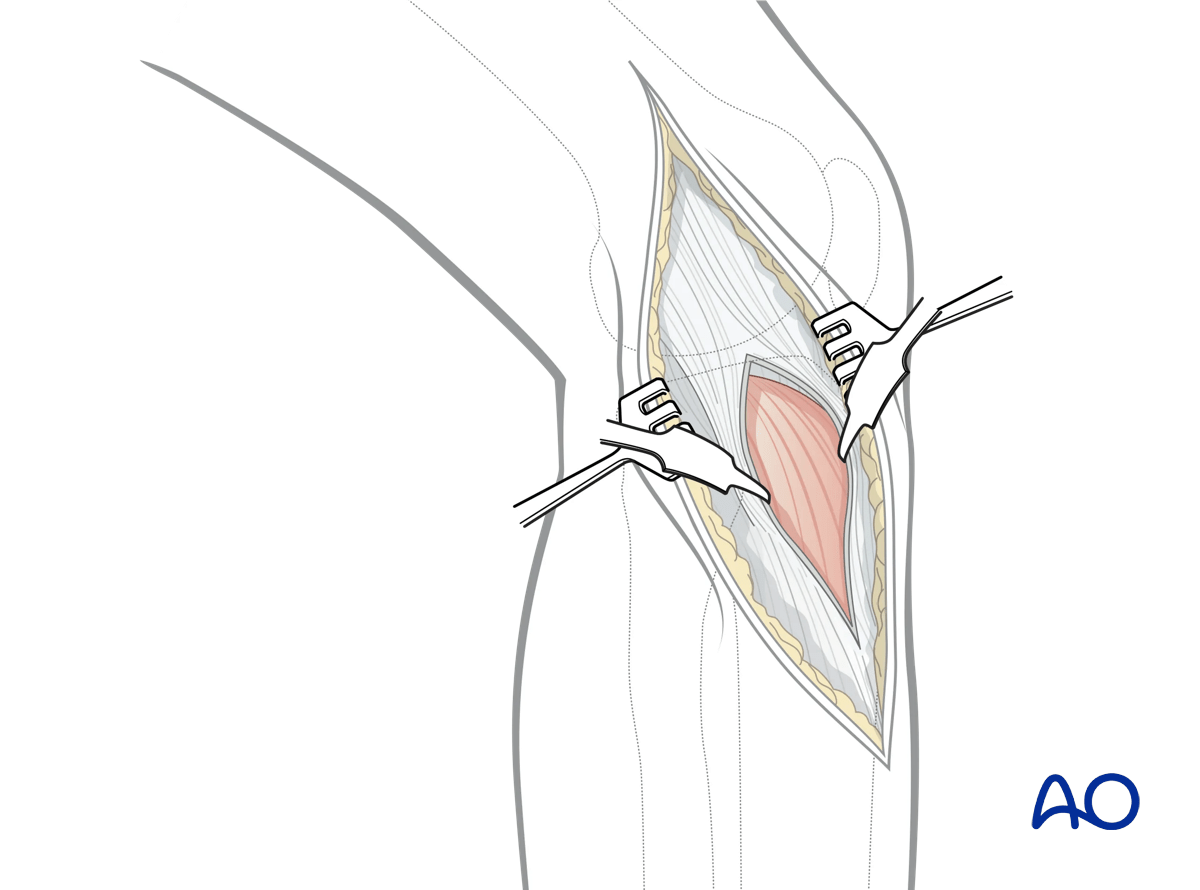
Release of the anterior compartment musculature from the lateral aspect of the proximal tibia is typically begun from distal to proximal. Dissection should be minimized to allow visualization of the fracture and the anticipated position of the plate.
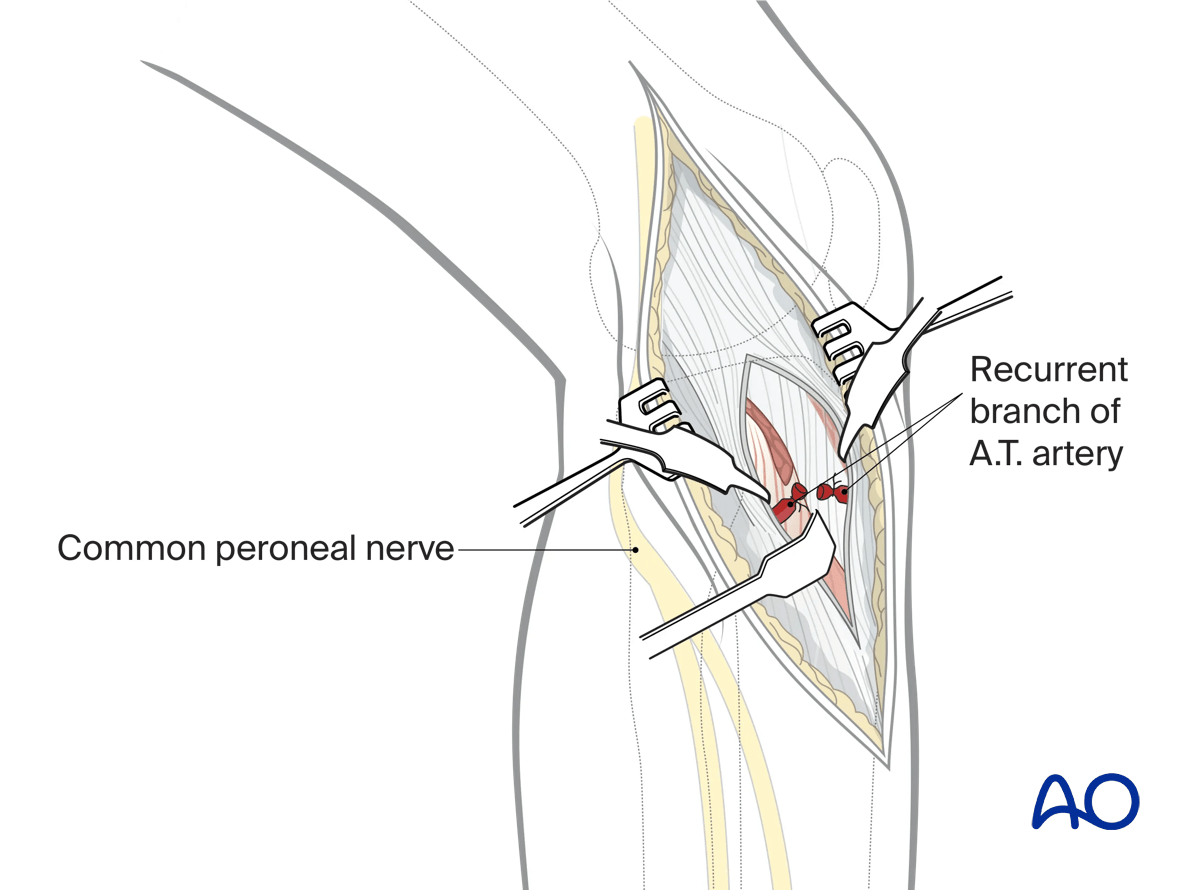
At the distal extent of Gerdy’s tubercle, and immediately adjacent to the osseous surface, the recurrent branch of the anterior tibial artery is universally encountered and can simply be cauterized.
The common peroneal nerve should not be encountered during this approach as it runs posterior to the surgical exposure.
4. Opening the joint
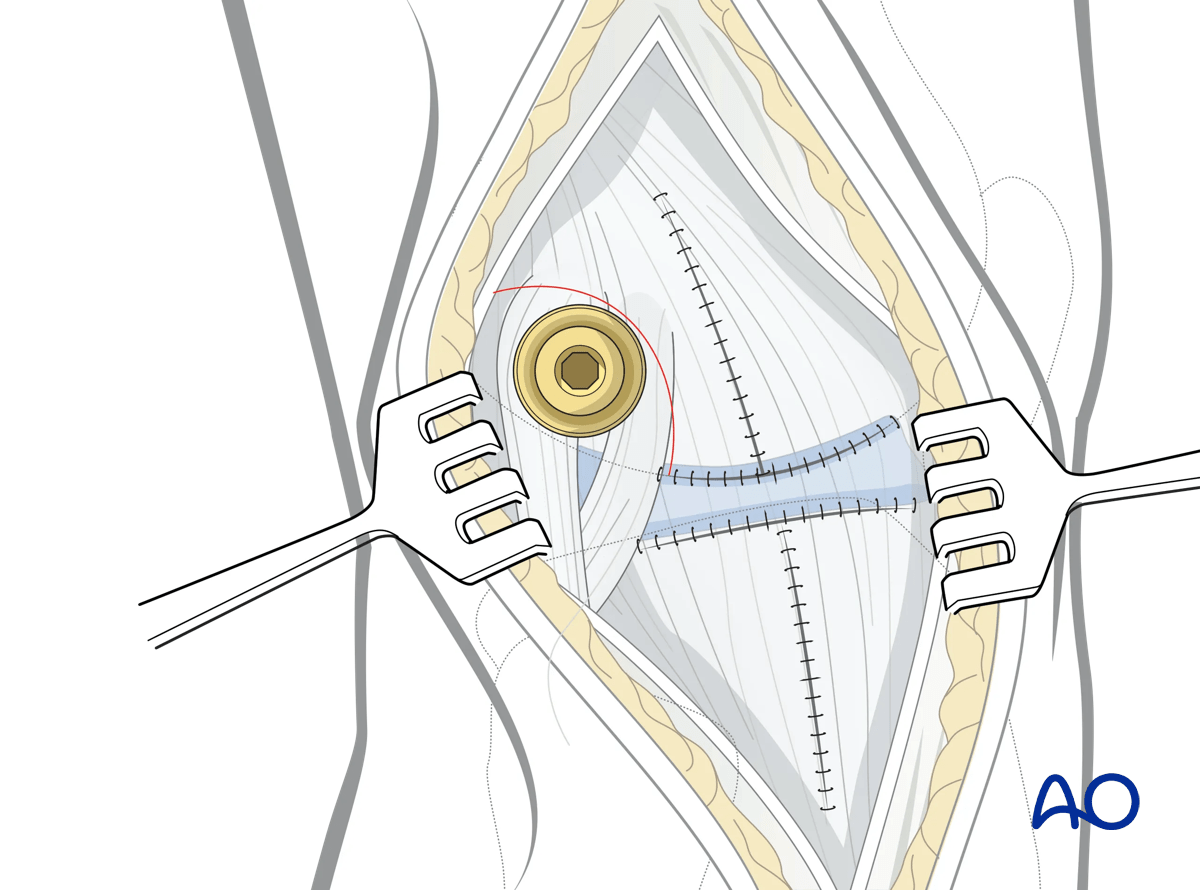
The lateral arthrotomy should be performed with joint distraction.
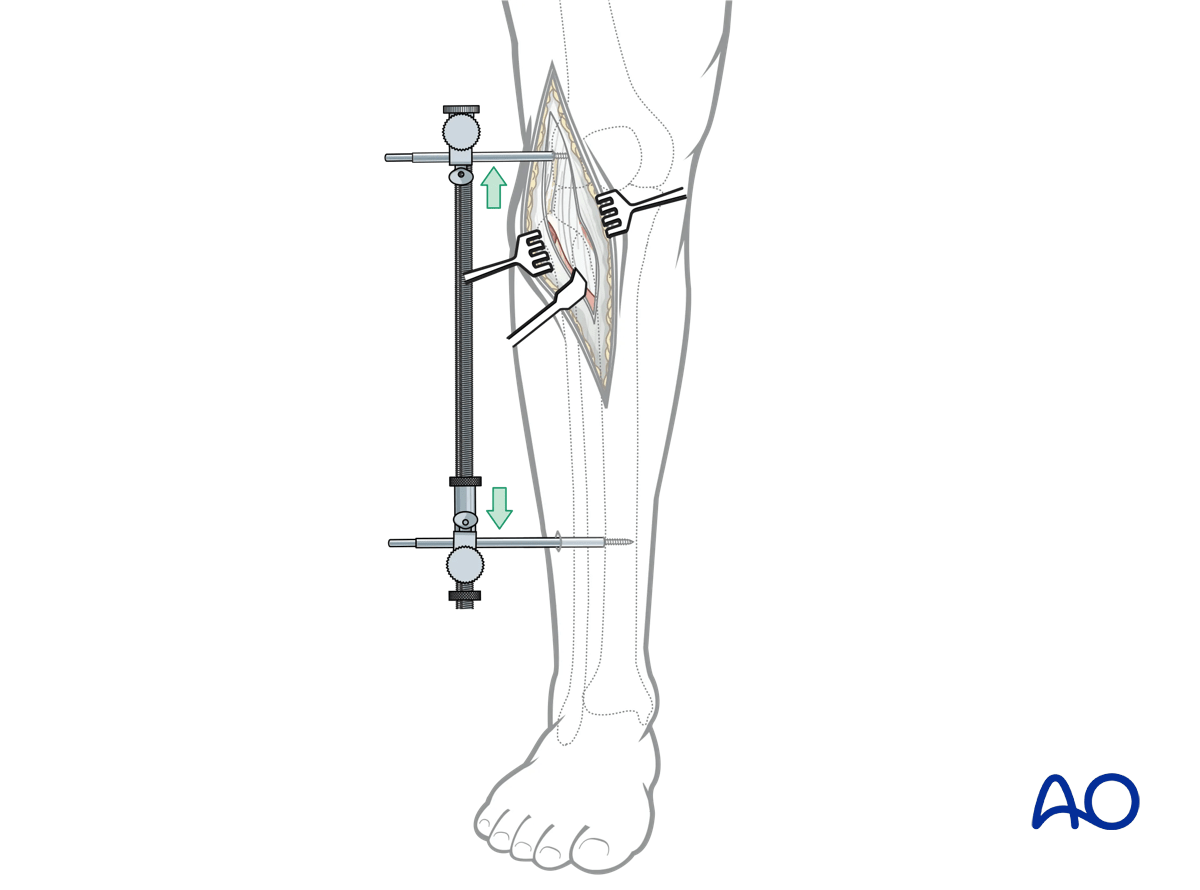
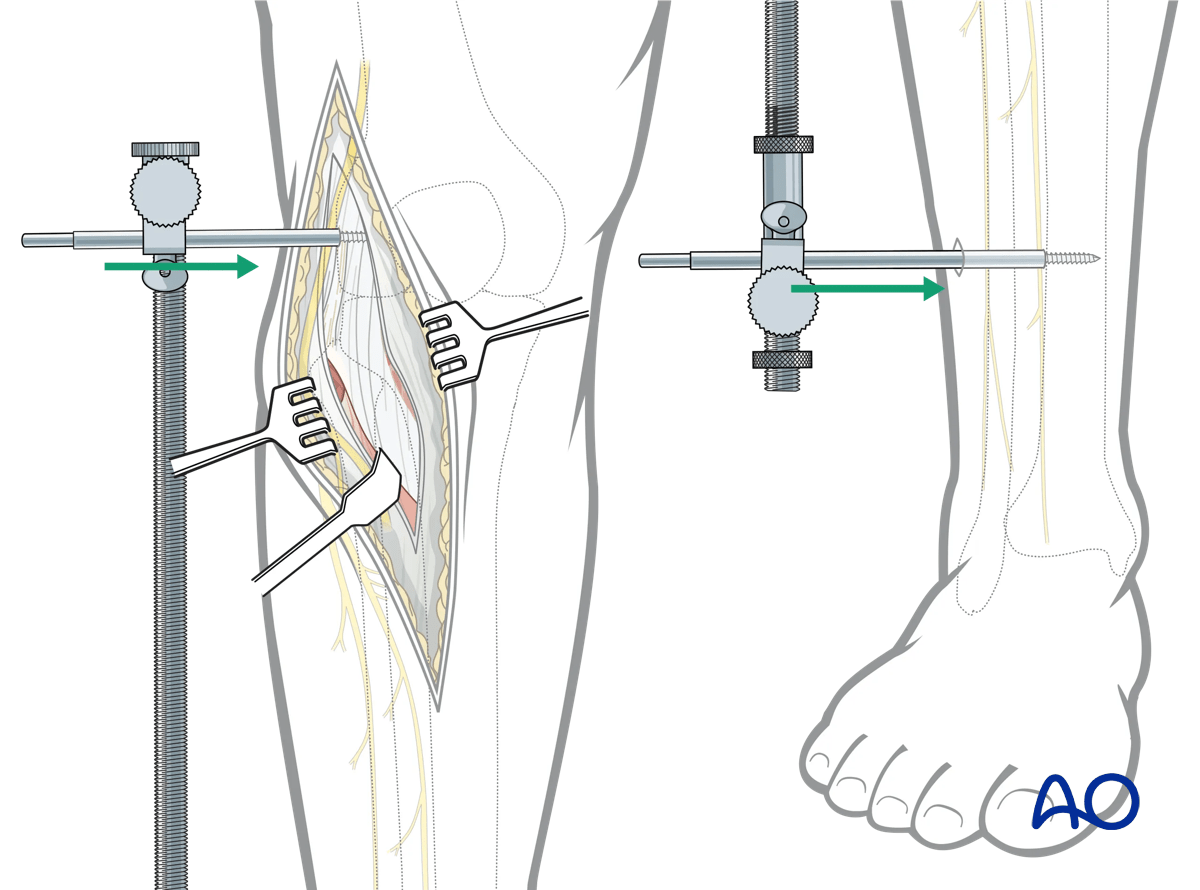
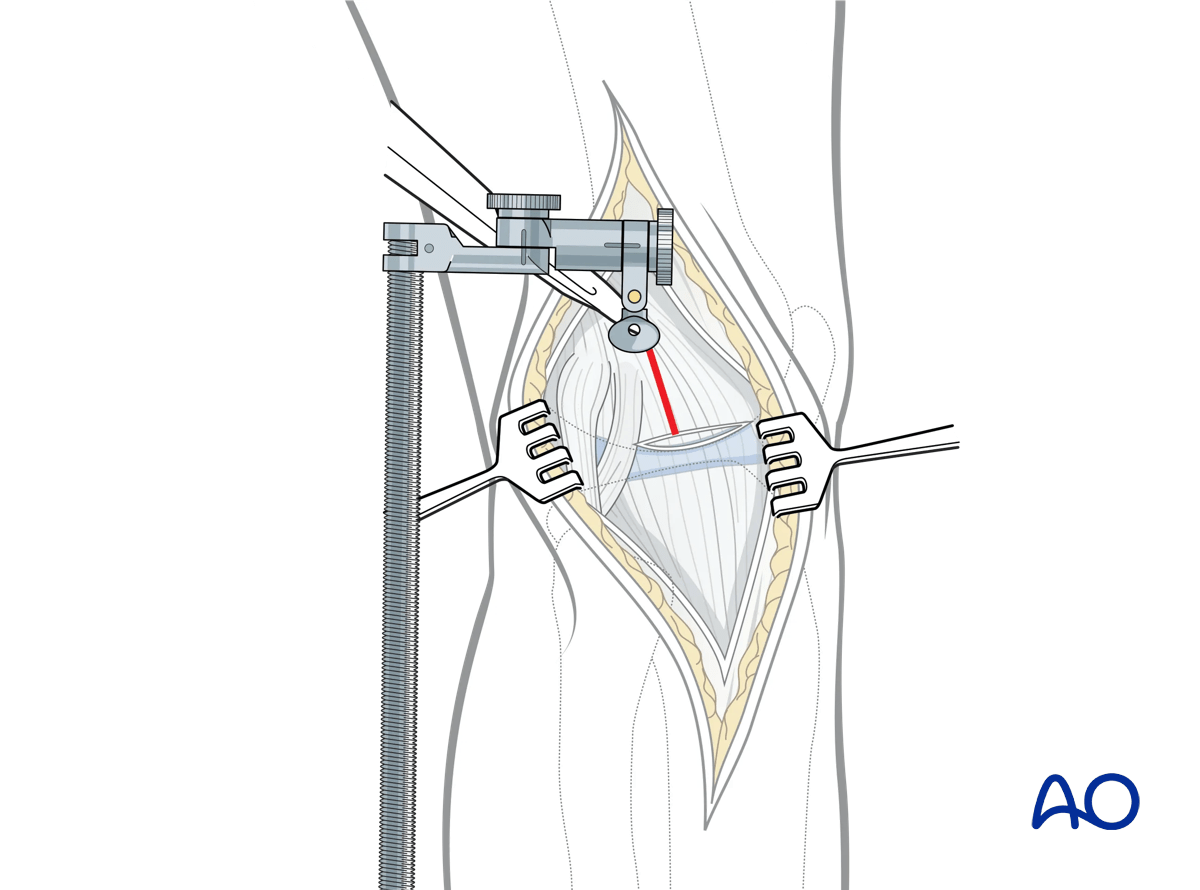
Application of the universal distractor
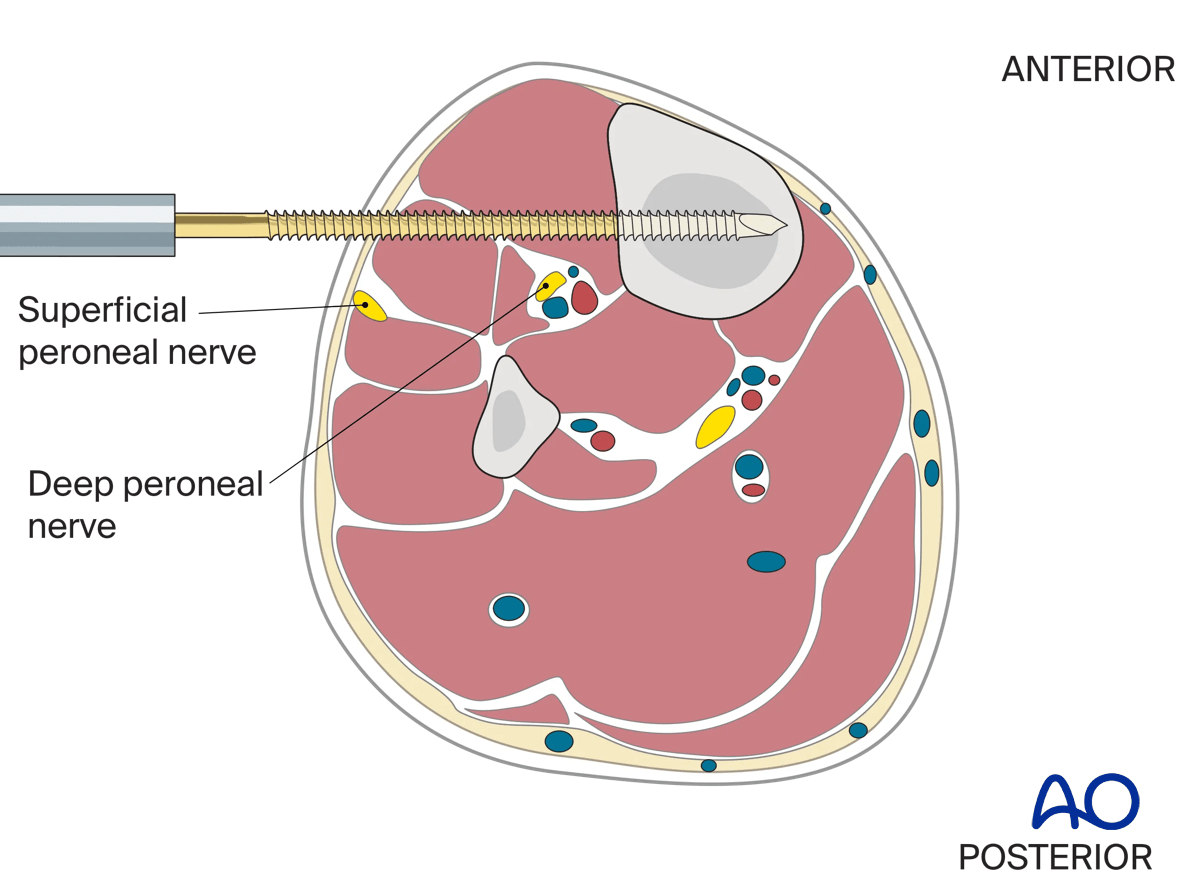
Through the proximal incision a lateral to medial 5 mm Schanz pin is inserted just proximal to the lateral epicondyle. A second Schanz pin is typically inserted percutaneously from lateral to medial in the distal tibial metadiaphysis out of the way of any anticipated implant placement. In very distal insertions care should be taken not to injure the superficial peroneal nerve. Both pins are typically placed bicortically. The universal distractor is then attached to the Schanz pins. The threaded bar is typically posteriorly-oriented. Care should be taken to ensure that the proximal mechanism of the femoral distractor does not obscure lateral fluoroscopic imaging. Distraction is then applied to the lateral column.
The risk to the superficial and deep peroneal nerves from placement of the distal pin are shown in this illustration.
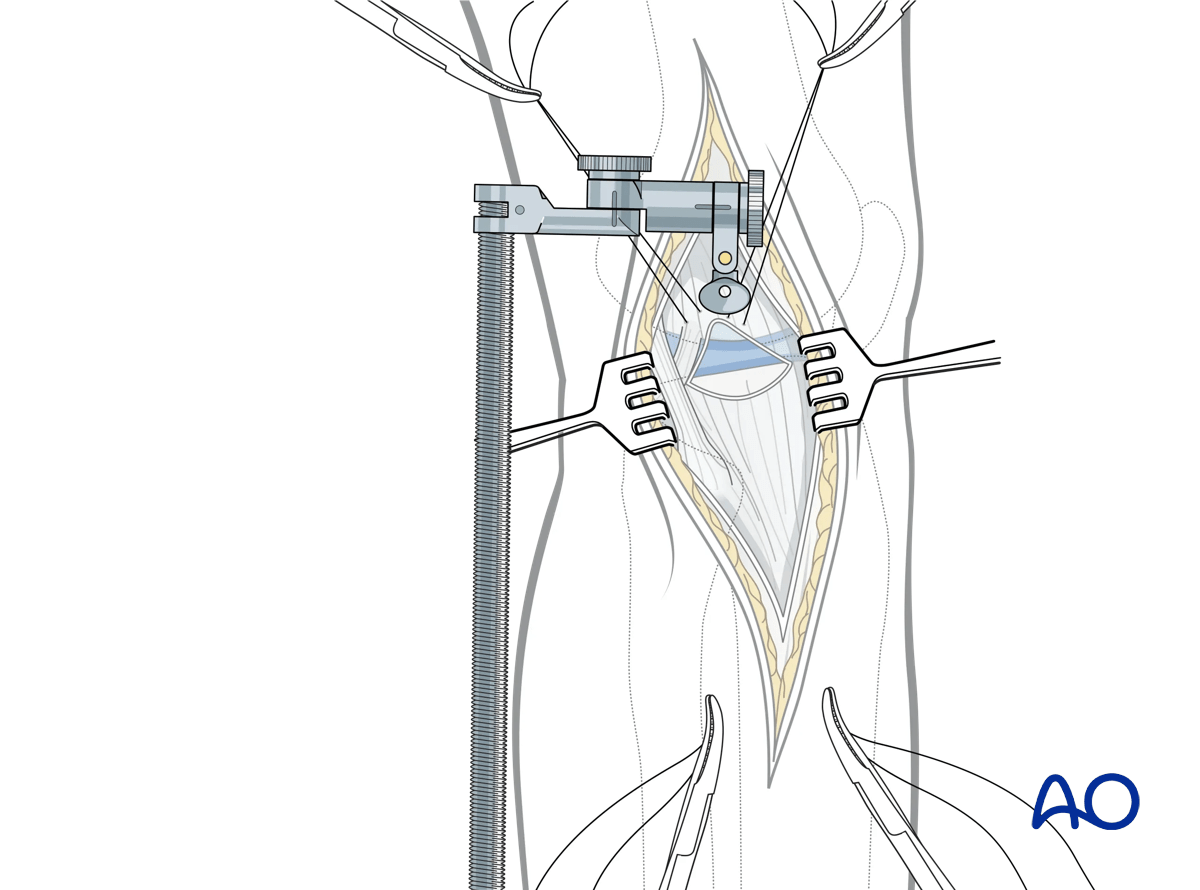
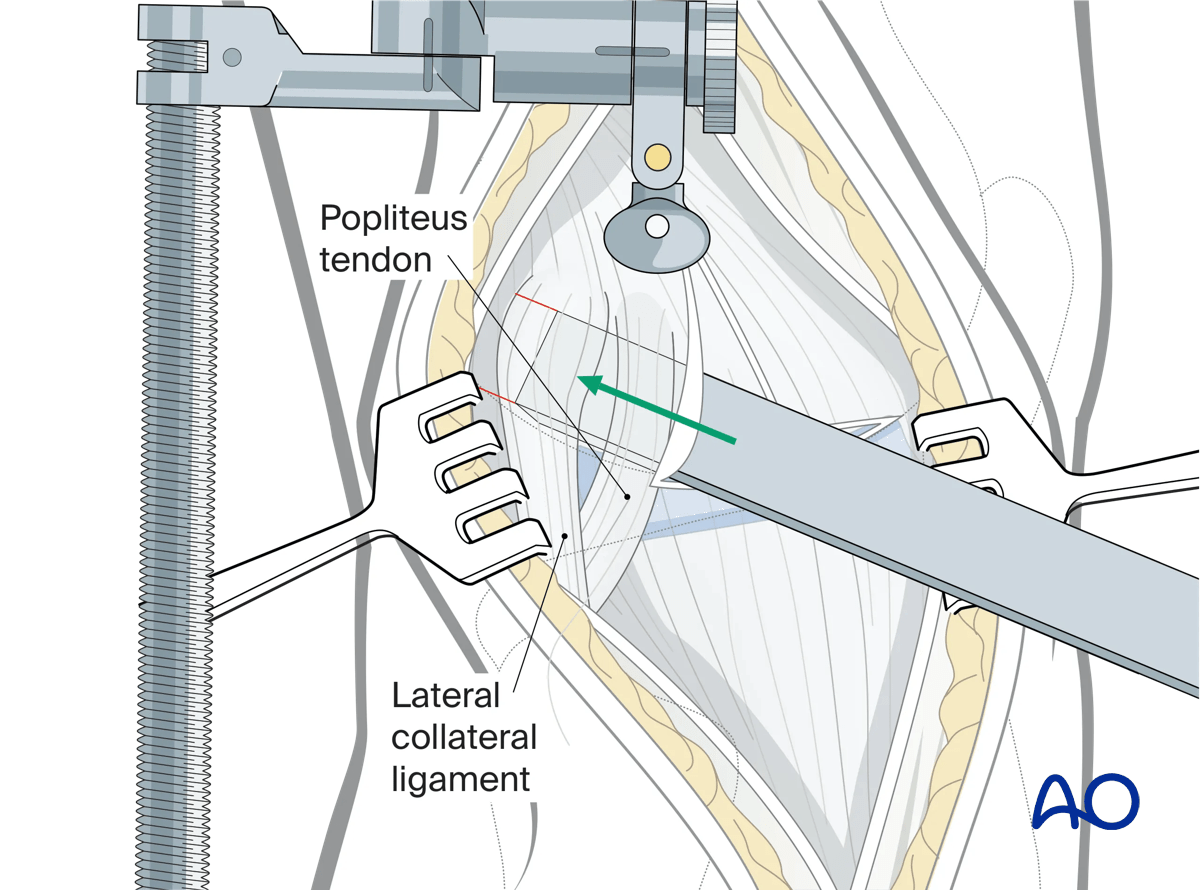
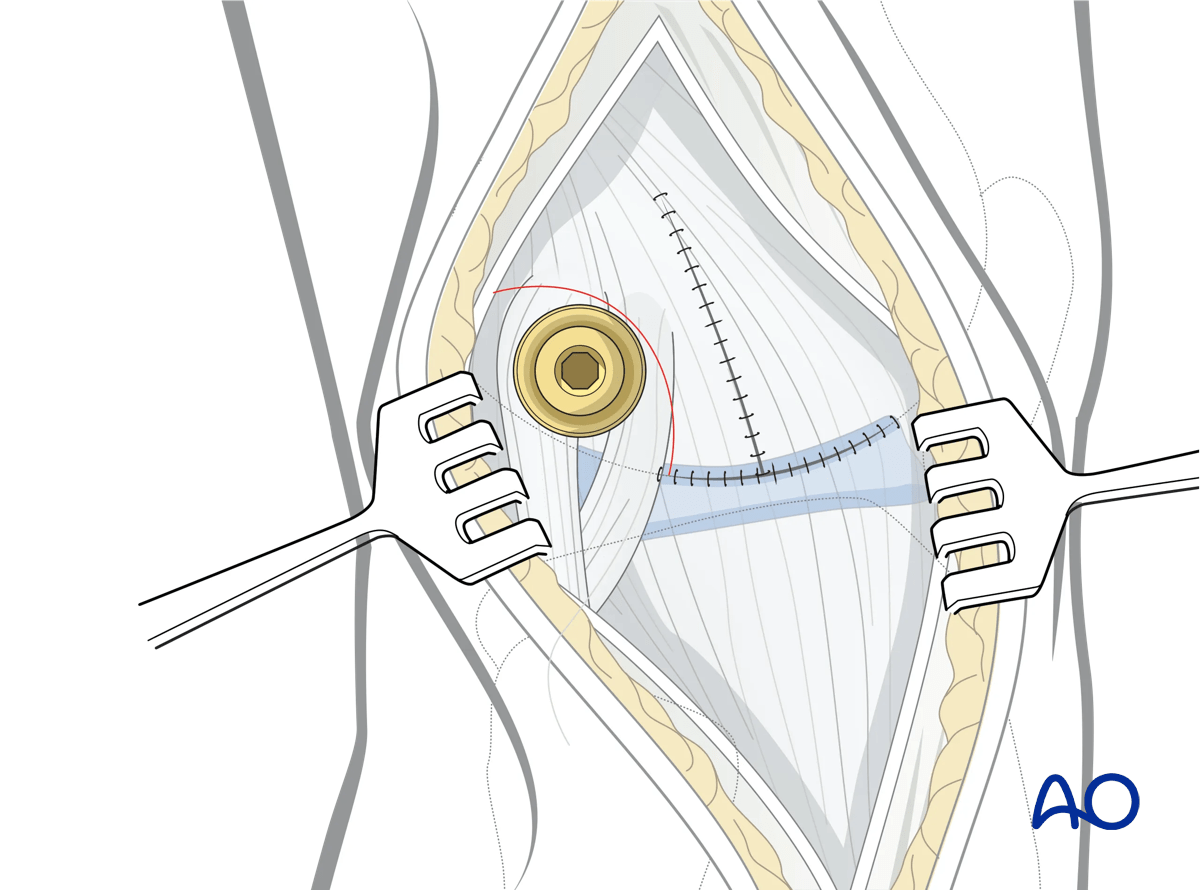
Arthrotomy
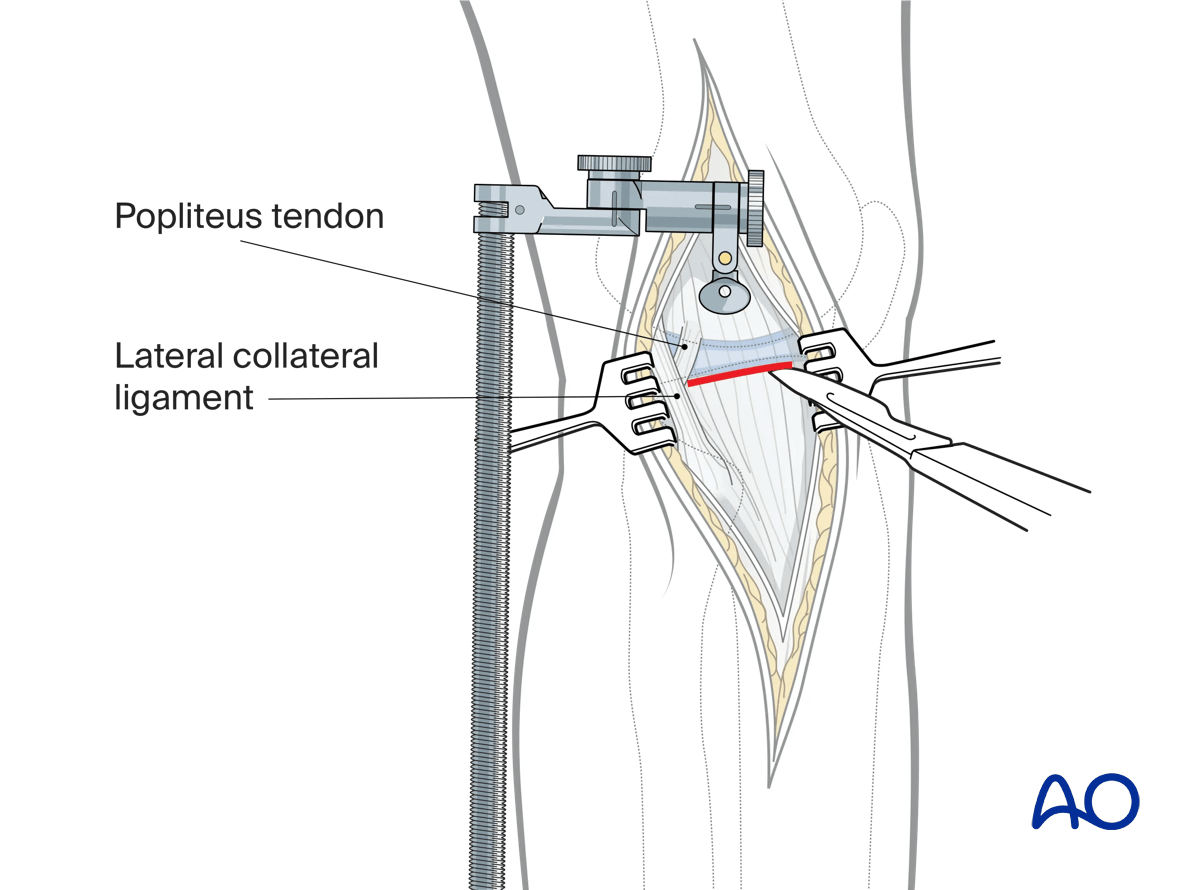
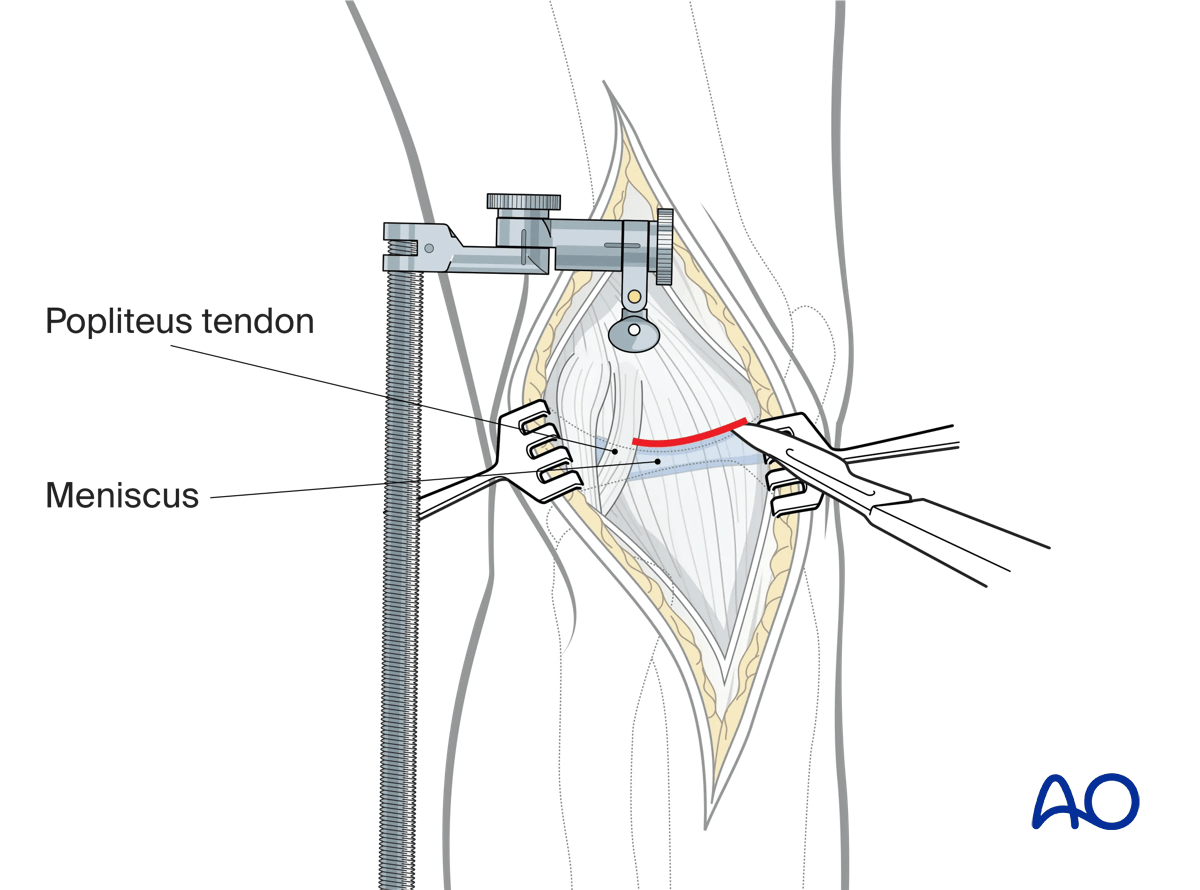
With the joint distracted, palpation can often identify the location of the lateral meniscus. A small submeniscal arthrotomy is then performed which typically reveals a hemarthrosis. Once the hemarthrosis is evacuated and the surgeon confirms that the arthrotomy truly is submeniscal the capsule can then be incised anteriorly and then posteriorly. The posterior capsulotomy is limited by the lateral collateral ligament (LCL) and the popliteus tendon (PT).
Joint visualization can be improved with the placement of a few retraction sutures at the lateral meniscal capsular junction.
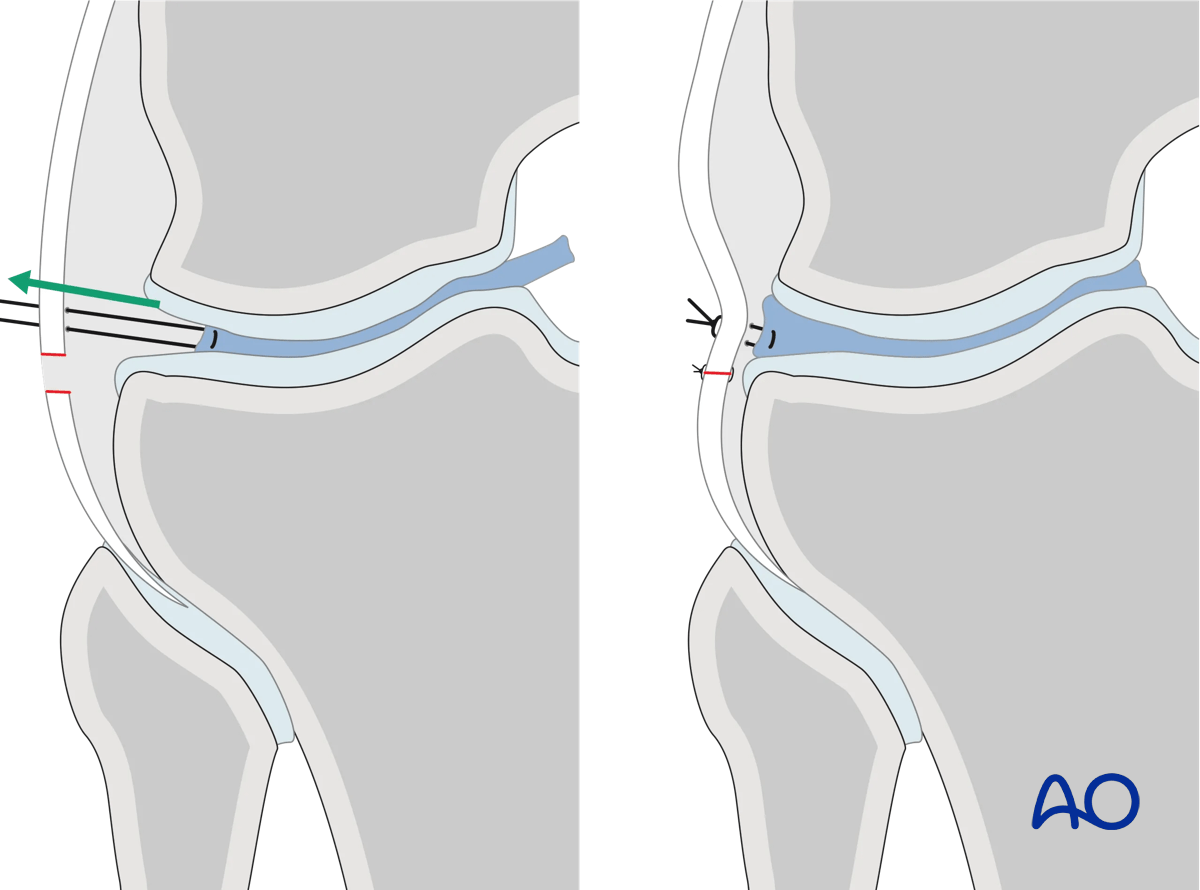
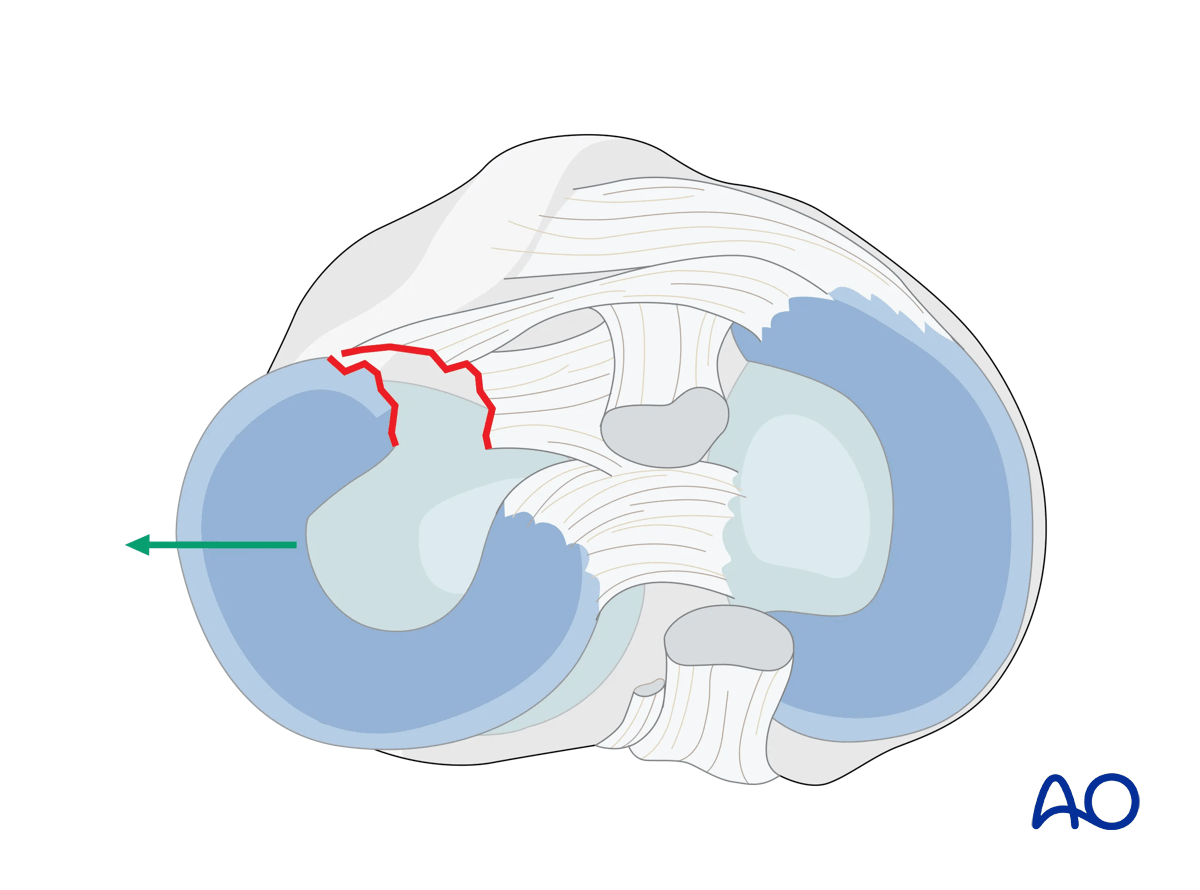
Lateral meniscal injuries associated with tibial plateau fractures are not uncommon. The typical injury is partial or complete peripheral detachment of the meniscus from the adjacent joint capsule. In some situations, the meniscus may lie with the depressed articular surface, or be entrapped by the split component. Failure to identify the meniscus upon joint arthrotomy should alert the surgeon to this possibility. Repair of the meniscus back to the capsule allows for appropriate visualization and management of the osteochondral surface and restoration of normal meniscal anatomy.
Meniscal repair is performed with an absorbable suture and placement of a series of simple mattress sutures. The suture is passed from external to internal through the joint capsule immediately at the location of the anticipated position of the superior aspect of the lateral meniscus. Once the needle is within the joint, it is then passed through the peripheral aspect of the torn meniscus from superior to inferior. The needle is then passed from internal to external through the joint capsule, but now at the distal extent of the anticipated location of the inferior border of the meniscus. The two ends of the suture can then be pulled, and the peripheral edge of the lateral meniscus should then be reapproximated to the inner aspect of the joint capsule. Three to five of these sutures are often placed symmetrically, reapproximating the torn peripheral edge of the lateral meniscus to the inner aspect of the joint capsule. The meniscal capsular junction is vascularized and healing in this area of the meniscus should occur.
5. Wound closure
The femoral distractor is removed. Closure of the submeniscal arthrotomy is performed, using absorbable suture. In situations where the capsular attachments to the tibia are deficient the proximal joint capsule can be reapproximated to the K-wire holes available in the majority of lateral tibial plateau plates.
The ilio-tibial band is then closed over the top of the lateral tibia plateau plate. Distal to Gerdy’s tubercle the anterior compartment fascia can be closed if there is no concern for significant postoperative swelling. In situations where there is significant concern, the surgeon has two options:
- Closure of the anterior compartment fascia with a subsequent anterior compartment fasciotomy performed lateral to the fasciotomy for surgical exposure.
- Leaving the anterior compartment fascia open. This option has a potential risk of leaving only skin and subcutaneous tissue closed over the internal fixation.
Dermal suture is used sparingly to reapproximate the skin. The skin is then closed with interrupted vertical mattress nylon suture or Allgower-Donatti suture.
6. Extended anterolateral approach
The extended anterolateral approach is infrequently utilized but can be very helpful. It provides improved visualization and manipulation of the posterior and posterocentral aspects of the lateral tibial plateau articular surface.
A transverse suprameniscal capsular incision is made above the lateral meniscus posteriorly from the PT hiatus towards the anterior horn. The capsule is now incised vertically towards the lateral epicondyle.
A vertical arthrotomy is carried out above the meniscus anterior to the lateral epicondyle.
The lateral epicondyle (and origin of the LCL) and the insertion of the PT (just distal and anterior to the lateral epicondyle) are identified. Using an appropriately-sized osteotome, the lateral epicondyle and insertion of the PT are osteotomized from the distal femur in an anterior to posterior direction. The epicondylar complex is reflected posteriorly.
The lateral meniscus is now handled in one of two ways. In situations where the anterior horn of the meniscus has been traumatically detached from the injury the meniscus can be reflected externally, and out of its intraarticular position.
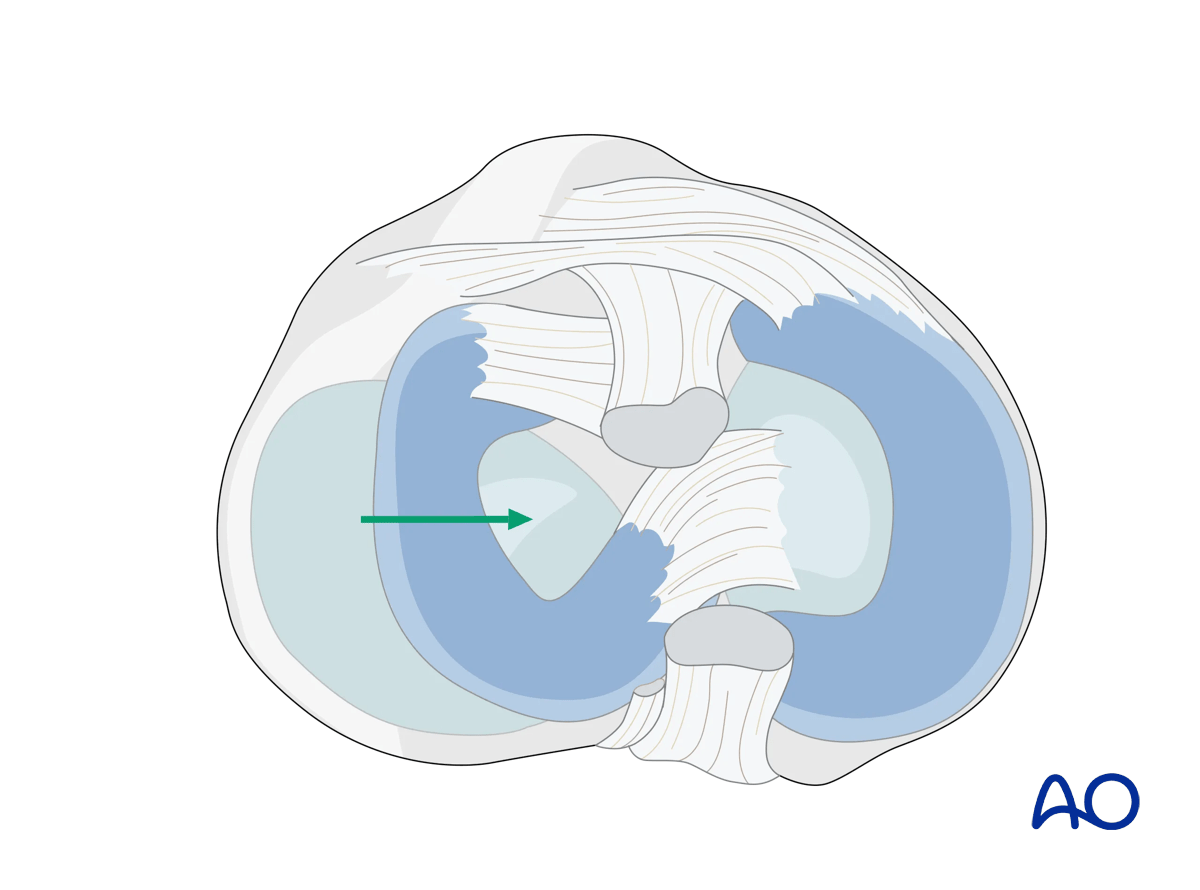
The second, more common, strategy, is to treat the meniscus as if it were subjected to a bucket-handle tear. In this situation the meniscus is entirely displaced intraarticularly toward the notch of the femur, effectively revealing the entirety of the lateral plateau articular surface.
Closure
The meniscus is relocated to its anatomic position. The osteotomized epicondyle and PT insertion are reduced to their anatomic locations and held with provisional wires. They are then definitively stabilized with a single screw and soft-tissue washer from lateral to medial.
The capsule is then reapproximated and the suprameniscal arthrotomy is closed.
Closure of the submeniscal arthrotomy stabilizes the lateral meniscus.