Suture fixation
1. Principles
Choice of fixation technique
Suturing is the best alternative to screw fixation if the avulsed fragment is small or comminuted. In the absence of suture anchor availability, sutures may be passed through drill holes in the proximal tibia.
Avulsion of the anterior cruciate ligament is most often seen in the younger patient.
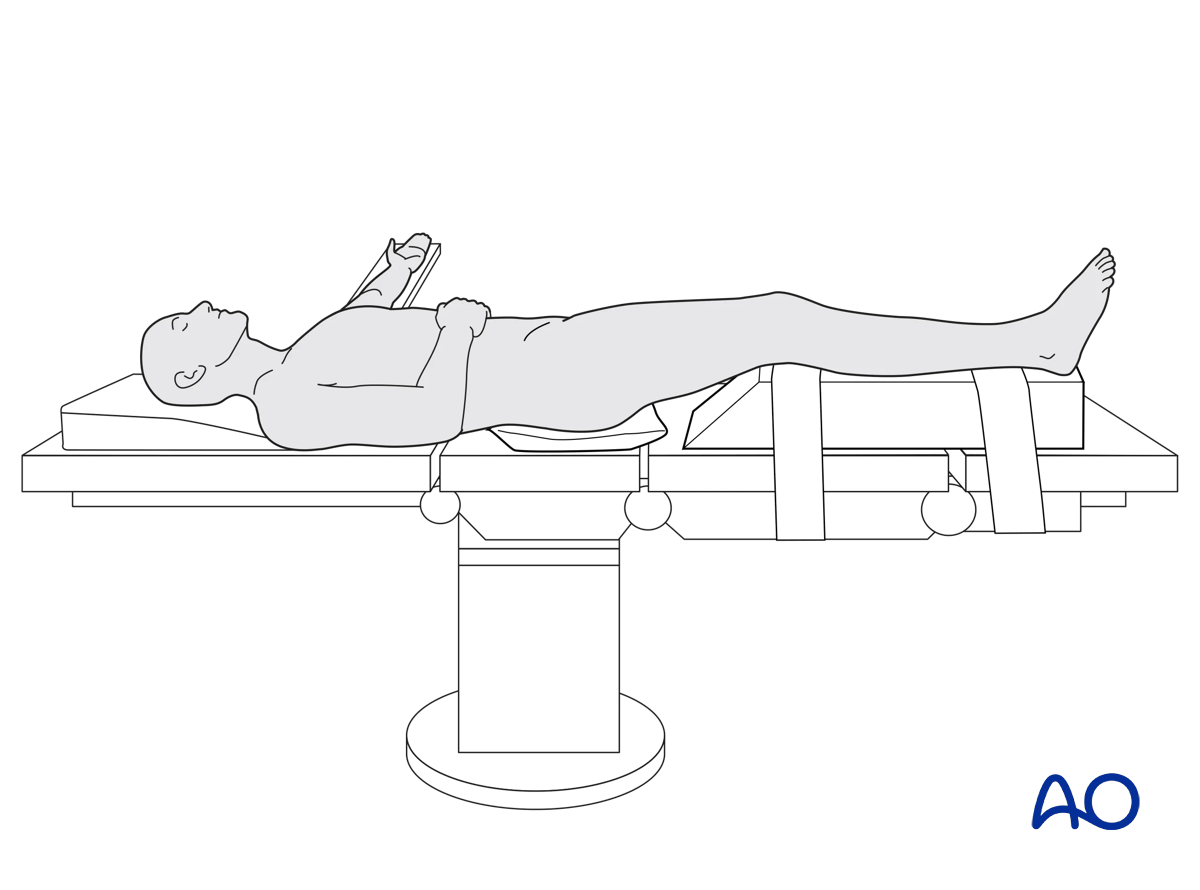
2. Patient preparation
This procedure is performed with the patient in a supine position.
3. Approaches
Depending on the fracture fragment size and location a small anteromedial or anterolateral parapatellar approach is used.
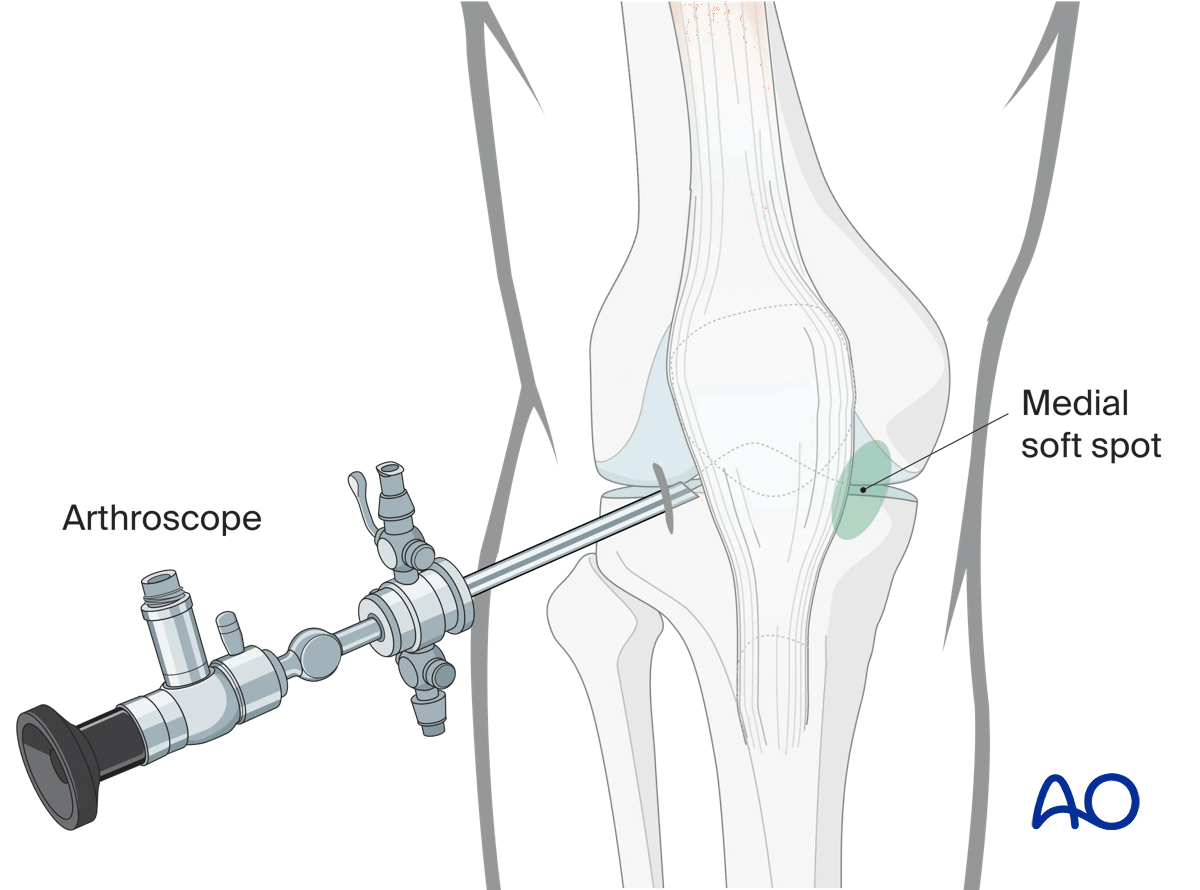
Arthroscopic approach to the knee
An arthroscopic approach may be used but advanced experience in arthroscopic surgery is essential.
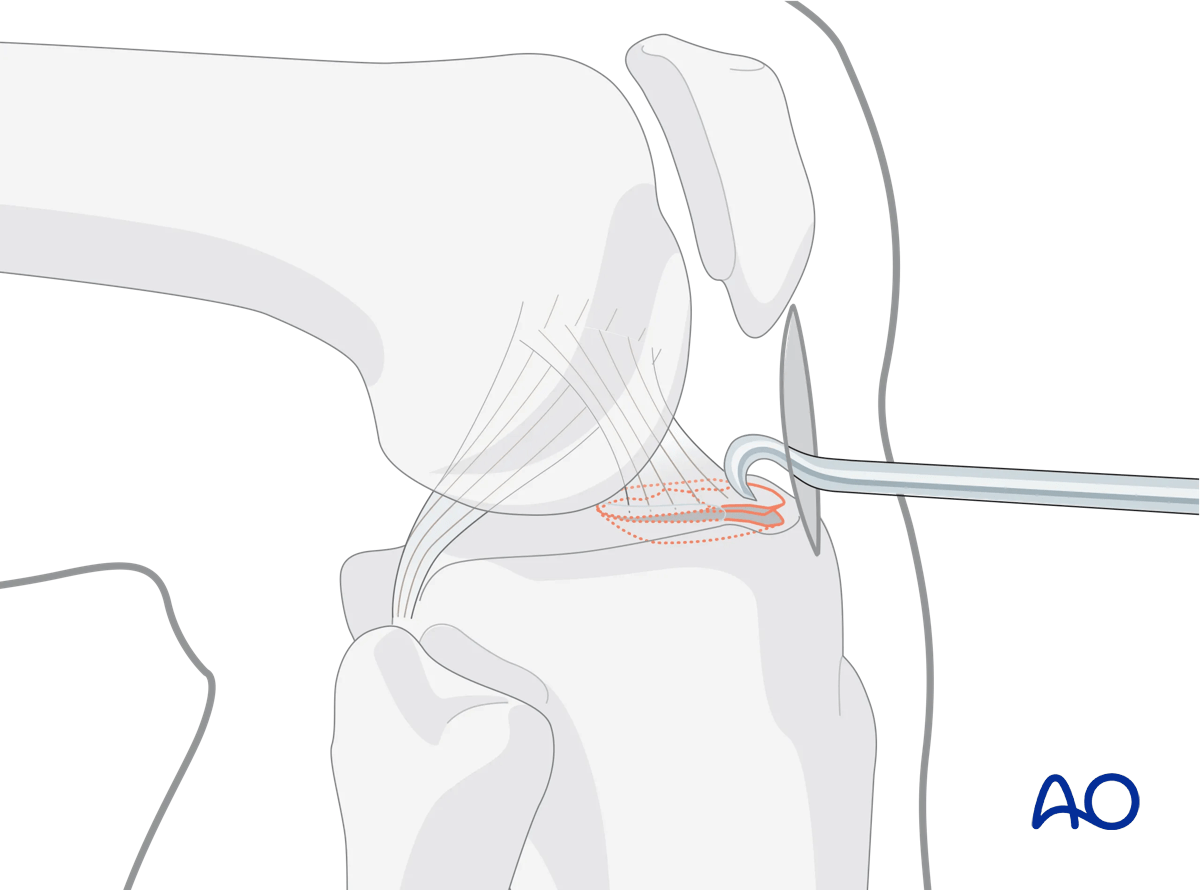
4. Reduction
Shoulder hook
In open procedures, the avulsed bony fragment of the intercondylar eminence is addressed directly and may be reduced with the help of a shoulder hook or wires.
5. Fixation
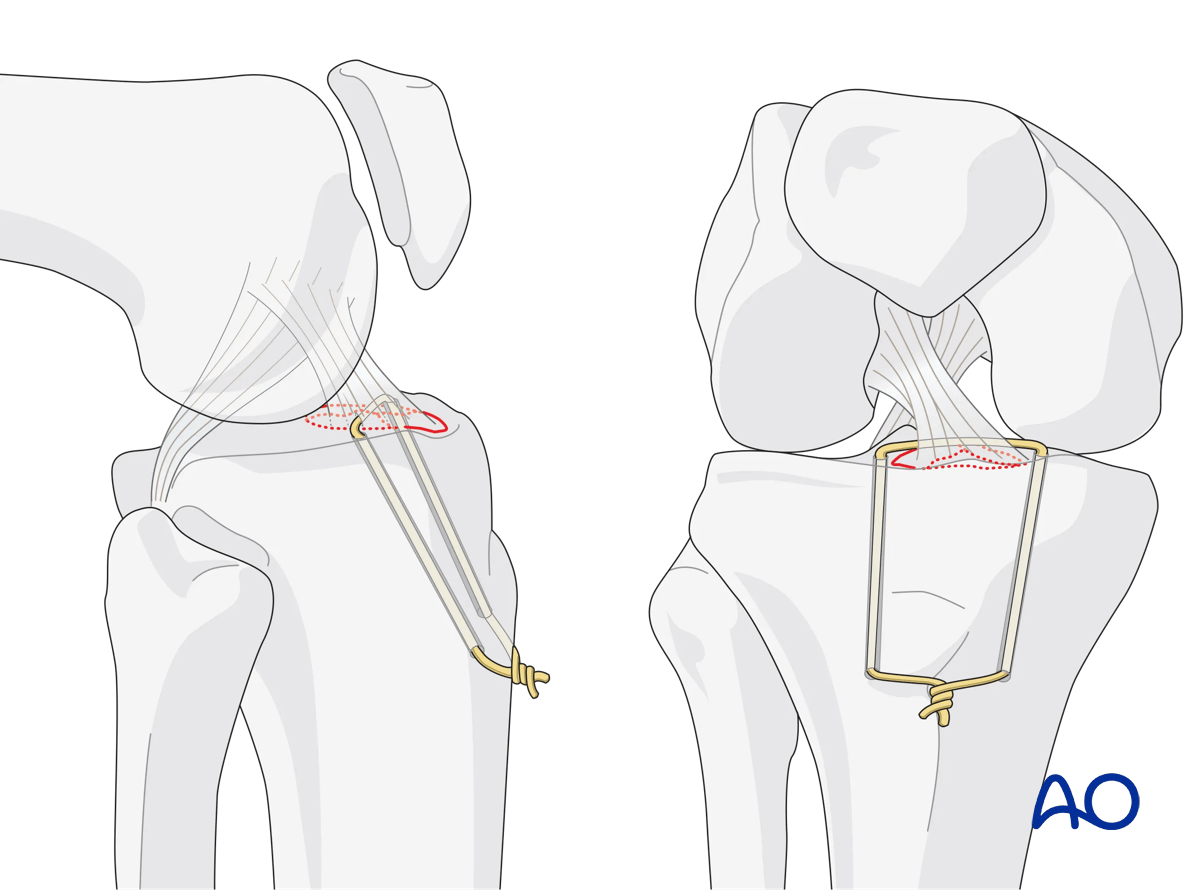
Drill holes
Two drill holes are placed retrograde into the anterior cruciate ligament (ACL) base, one medial and one lateral.
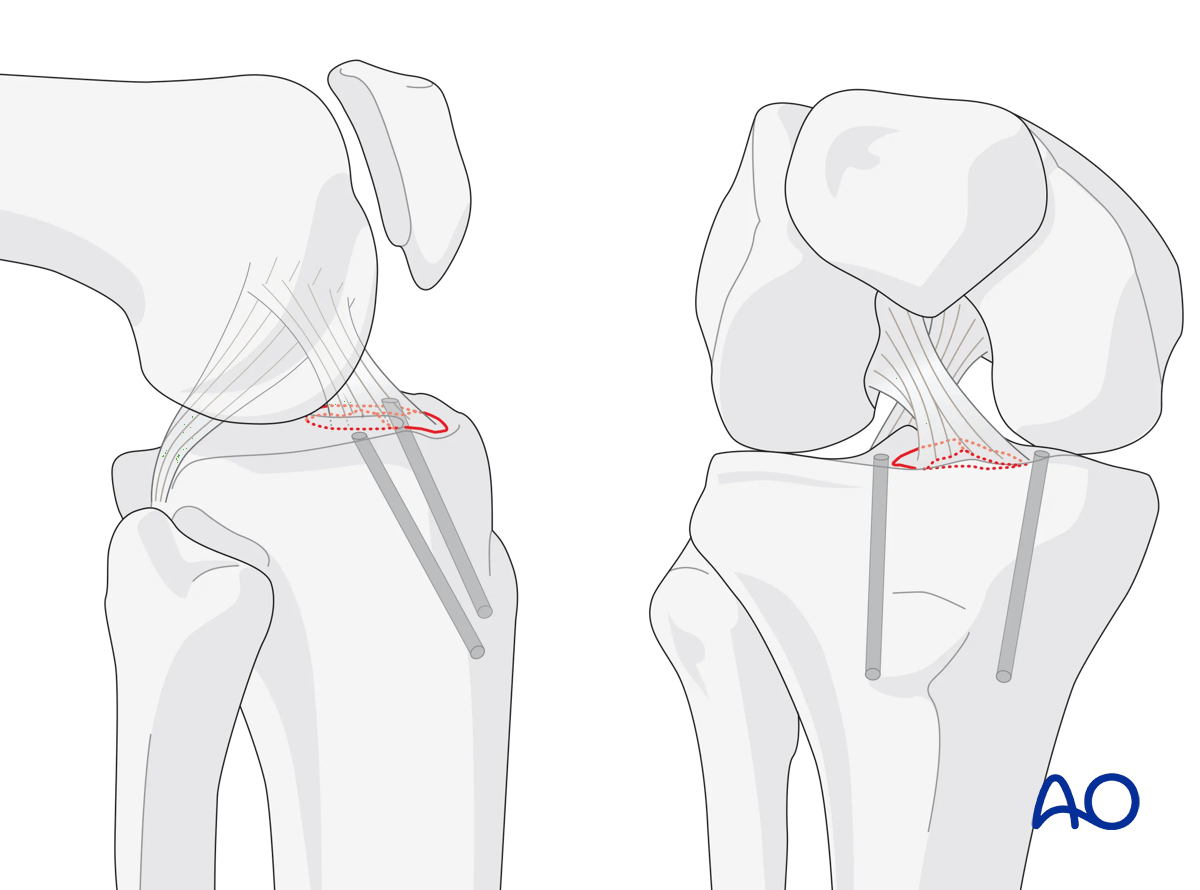
Apply suture
Place the sutures around the base of the ACL, pass them through the holes, make a knot, and tighten it.
6. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













