Angular stable plating
1. Principles
Angle stable fixation has evolved from a technique using self-drilling, self-tapping unicortical screws. The original concept largely centred on using the implant as an internal fixator, often intended as being placed using minimally invasive insertion and associated with indirect reduction methods.
Currently, numerous angle stable fixation devices demonstrate improved periarticular design, the ability to use combinations of both cortical and variable-angled locking screws, and placement can be done using open or minimally invasive/percutaneous methods. These features allow the plate to be used as a reduction tool helping to achieve metadiaphyseal alignment, facilitating buttressing of meta-epiphyseal fracture fragments, while still allowing angular stability to provide enhanced stability and fracture bridging when needed or desired.
Stability created by conventional plating requires friction between the surface of the bone and the plate. This requires conventional screws to create tension along the screw axis. The more the screw can be tightened, the greater the axial tension in the screw, and the greater the friction created between the plate and bone. In osteoporotic bone, where the screw cannot create enough axial tension, the friction of the plate to the bone is decreased and screws loosen easily, jeopardizing stability between the plate and the bone.
Many angle-stable plates now offer variable angle locking, which allows the surgeon to have some determination of screw trajectory, yet still have the ability to lock. It is worth noting that there will be a nominal position where the locking mechanism has optimal stability. Deviations from this often result in a decrease in stability of the locking mechanism but allow the freedom of avoiding predetermined screw trajectory.
The original device was particularly helpful for percutaneous minimally invasive indirect reduction treatment, and this will be shown illustrated in coverage of A-type injuries. Current locking designs are illustrated in partial and complete articular fractures.
2. Preoperative planning
Screw type
In cases of healthy bone structure, unicortical angle-stable screws seem to provide clinically satisfactory stability when cortical bone is normal. However, with significant osteoporosis the torsional and angular stability of the unicortical screw is compromised, as there is a short working length of the screw in the bone. Placement of bicortical screws increases the torsional and angular stability substantially, regardless of the density of the cortex in all situations.
3. Patient preparation
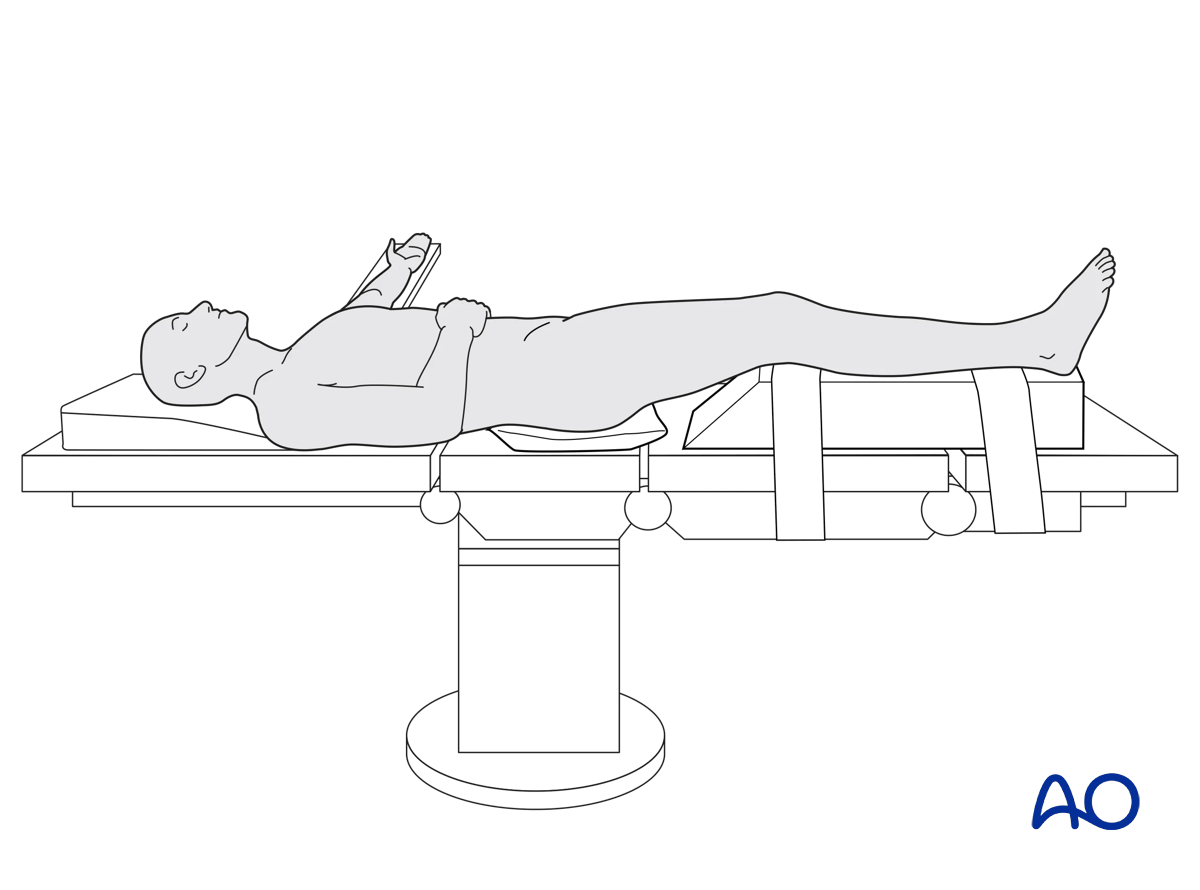
This procedure is normally performed with the patient in a supine position.
4. Approach
Anterolateral approach
The proximal portion of the anterolateral approach is utilized, limiting the incision and deep dissection to just proximal and just distal to Gerdy’s tubercle. Undue skin tension or prolonged soft tissue compression should be avoided. Screws placed distal to the proximal exposed portion of the plate are necessarily placed percutaneously, or with small incisions. Many systems offer external targeting jigs and soft-tissue sleeves to protect the soft tissues during drilling, measuring, and screw placement.
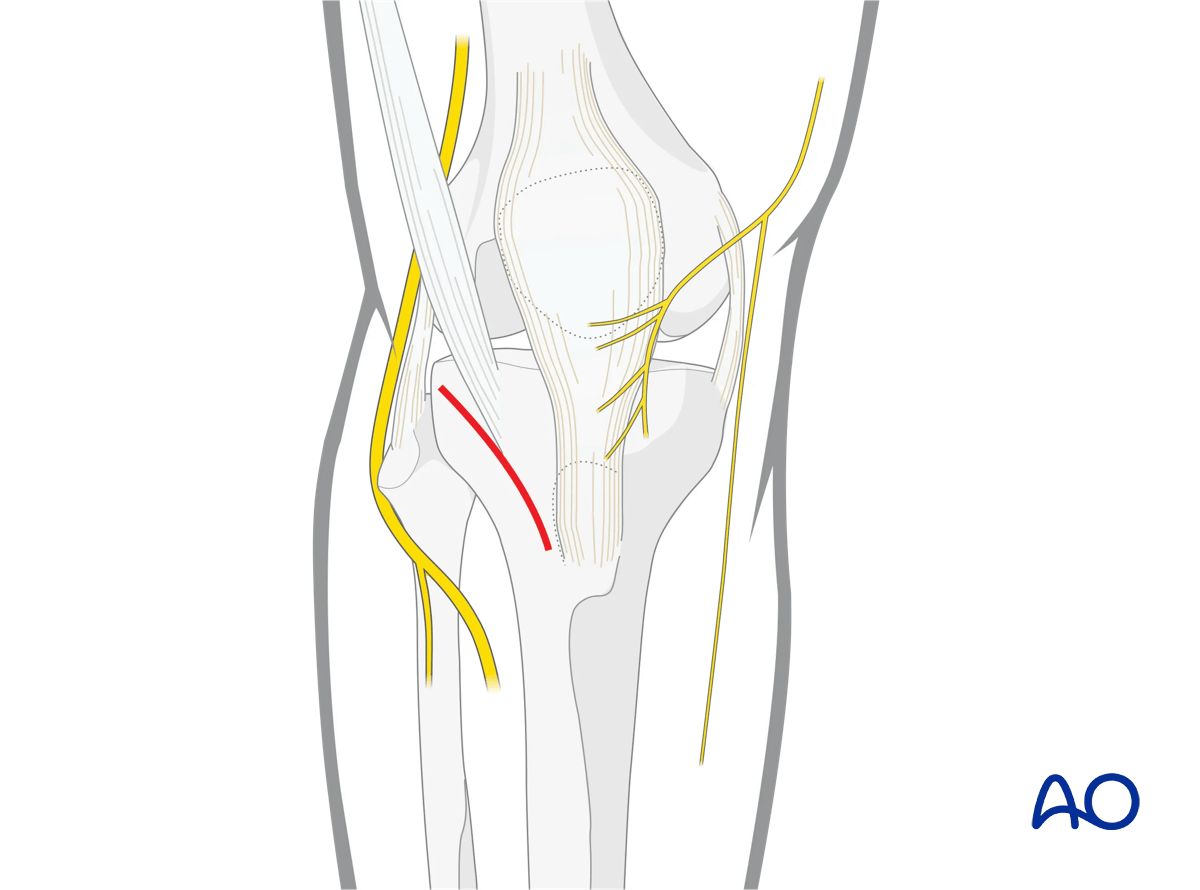
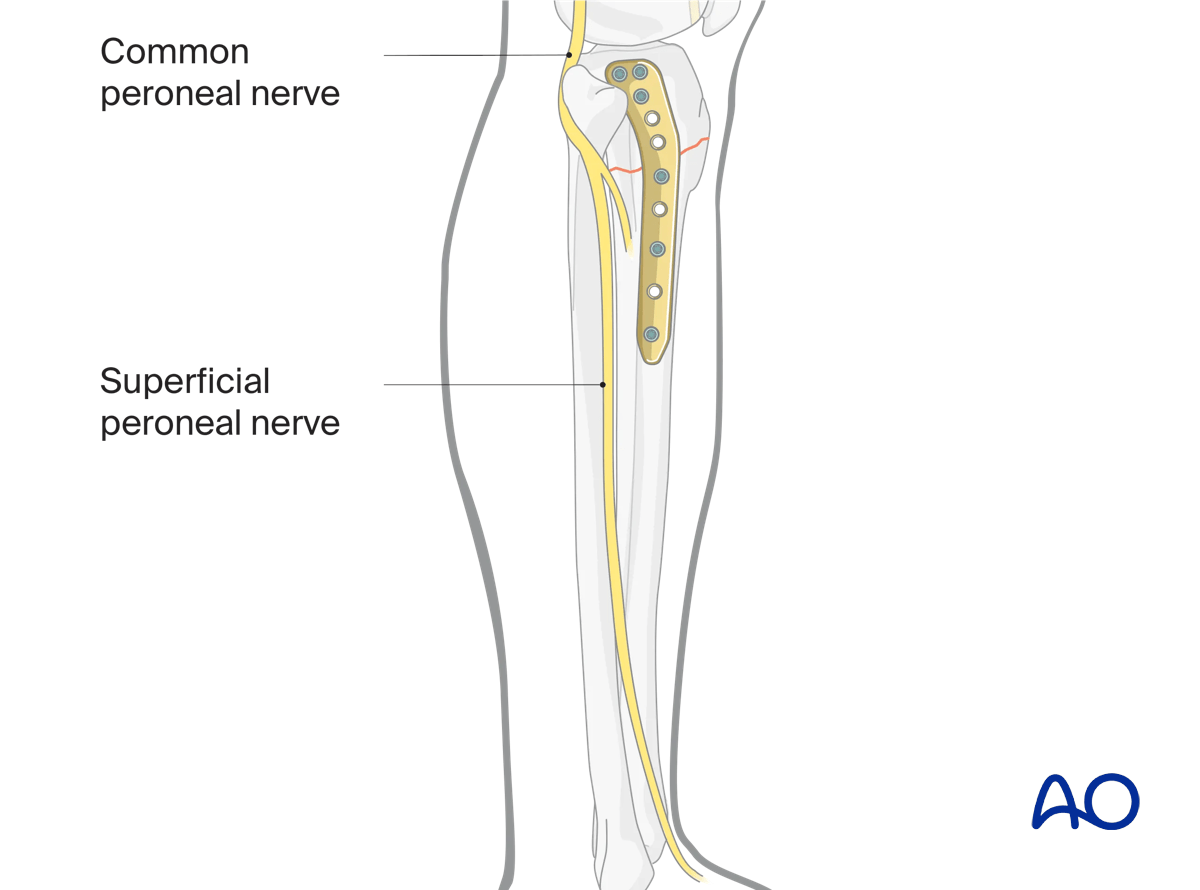
The surgeon must still be aware of local anatomical hazards, particularly the anterior tibial neurovascular bundle and superficial peroneal nerve.
The superficial peroneal nerve is a structure at risk when plating reaches the distal quarter of the tibia laterally. When using percutaneous techniques in this region a slightly elongated distal incision is useful both to check plate location and avoid damage to superficial peroneal nerve branches.
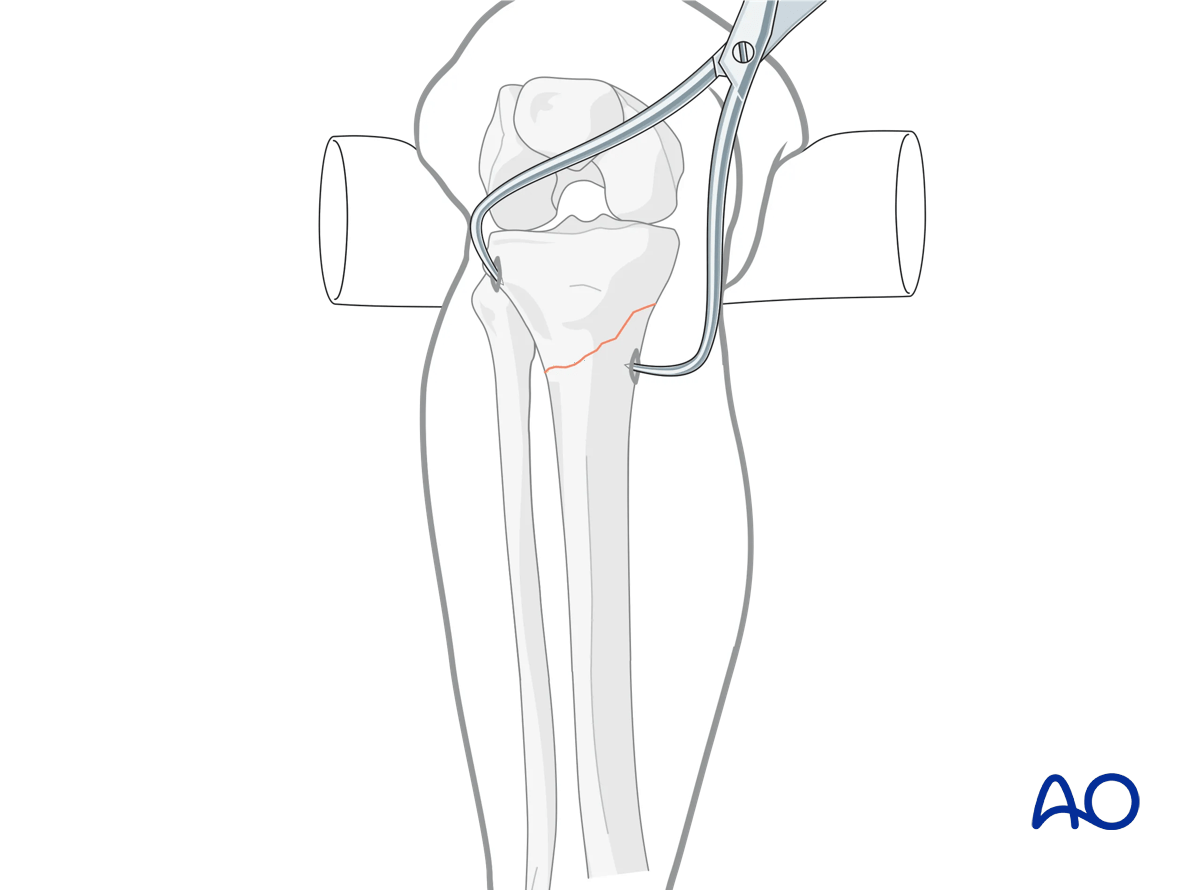
5. Reduction
An open exposure, direct visualization, and anatomic reduction should be performed for simple fractures. The fracture is reduced in a soft-tissue friendly manner, using the appropriate clamps, and direct reduction maneuvers, the same as one would do with conventional plating. Any interfragmentary compression should be performed prior to inserting locking screws on either side of the fracture.
6. Fixation
Plate insertion
Once the fracture is provisionally reduced the plate may be placed in an antegrade, submuscular fashion. Plates with a blunt, beveled distal end do not require pathway preparation along the lateral aspect of the tibia. In some situations, the passage of a Cobb elevator may facilitate subsequent plate placement. If a targeting jig is used the accuracy of targeting should be assured prior to plate placement.
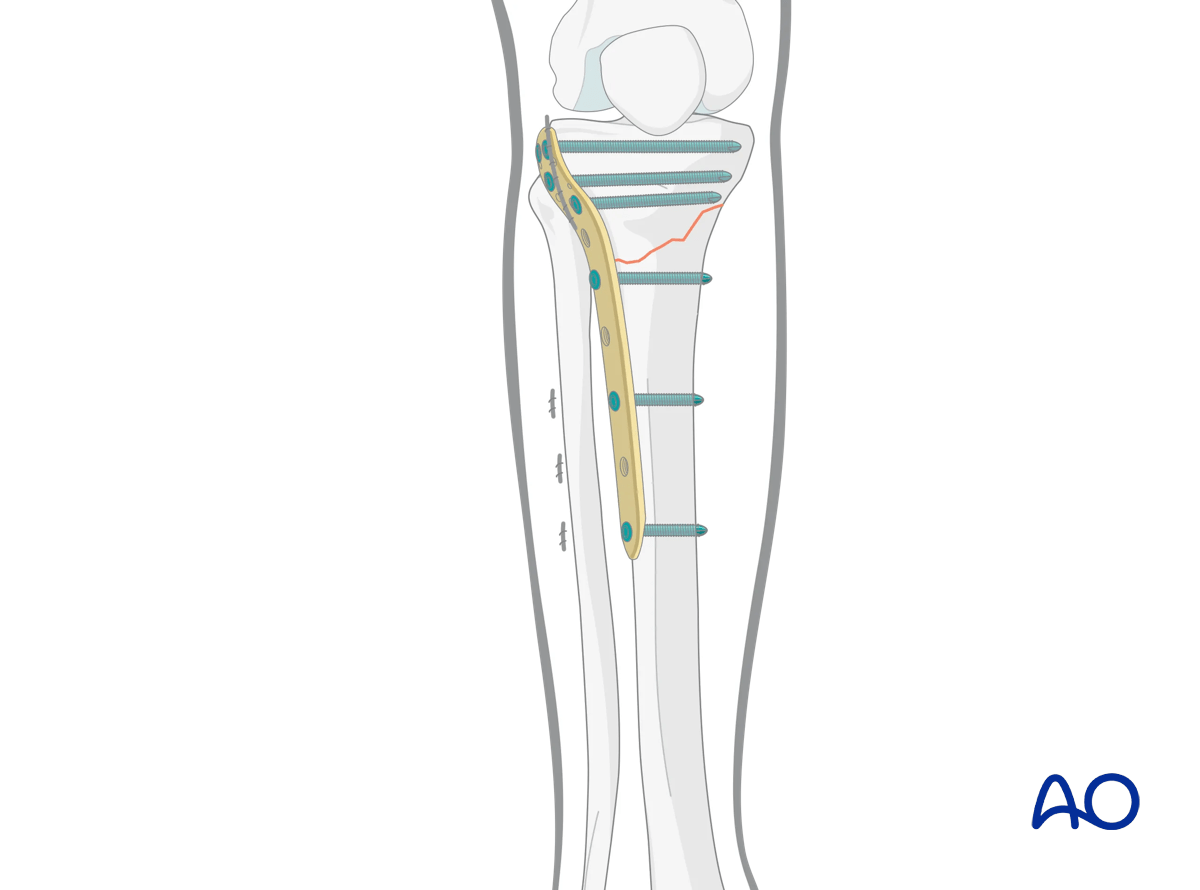
Positioning of the plate
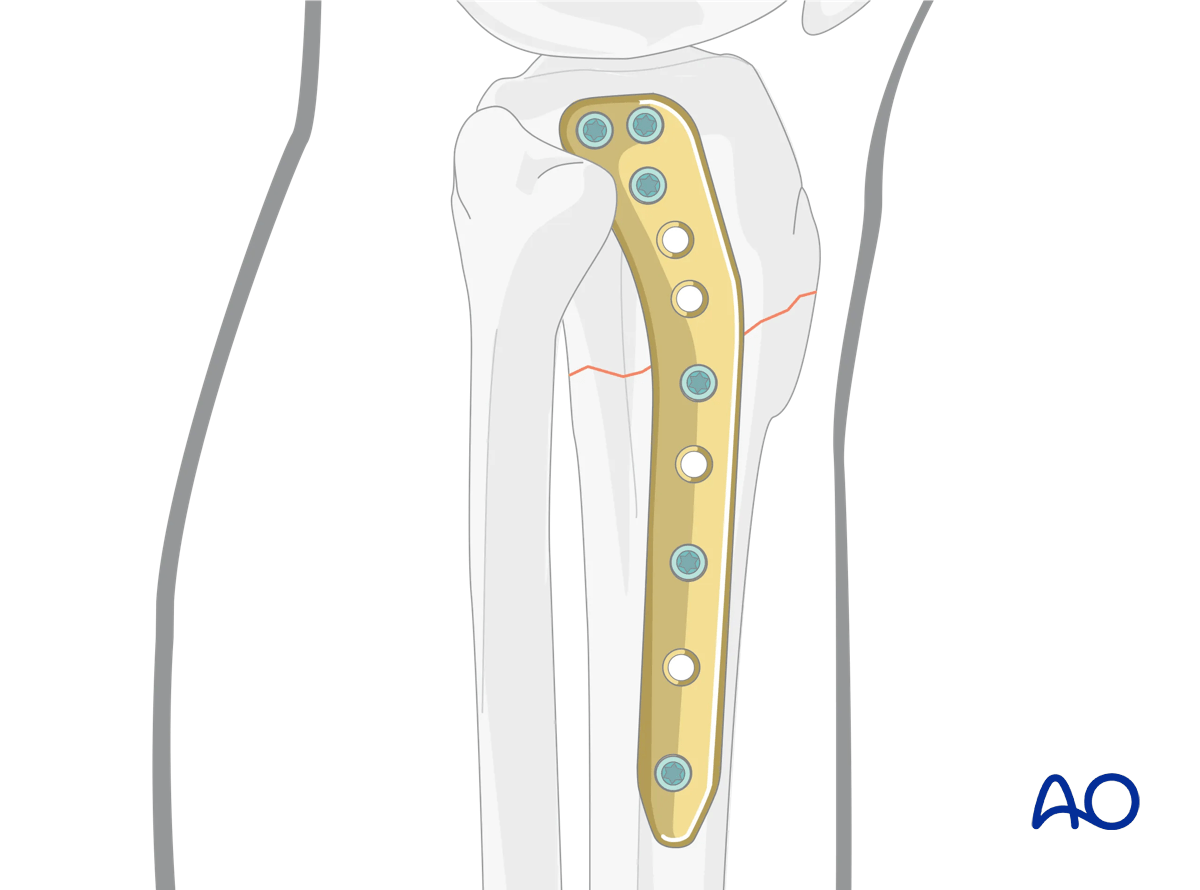
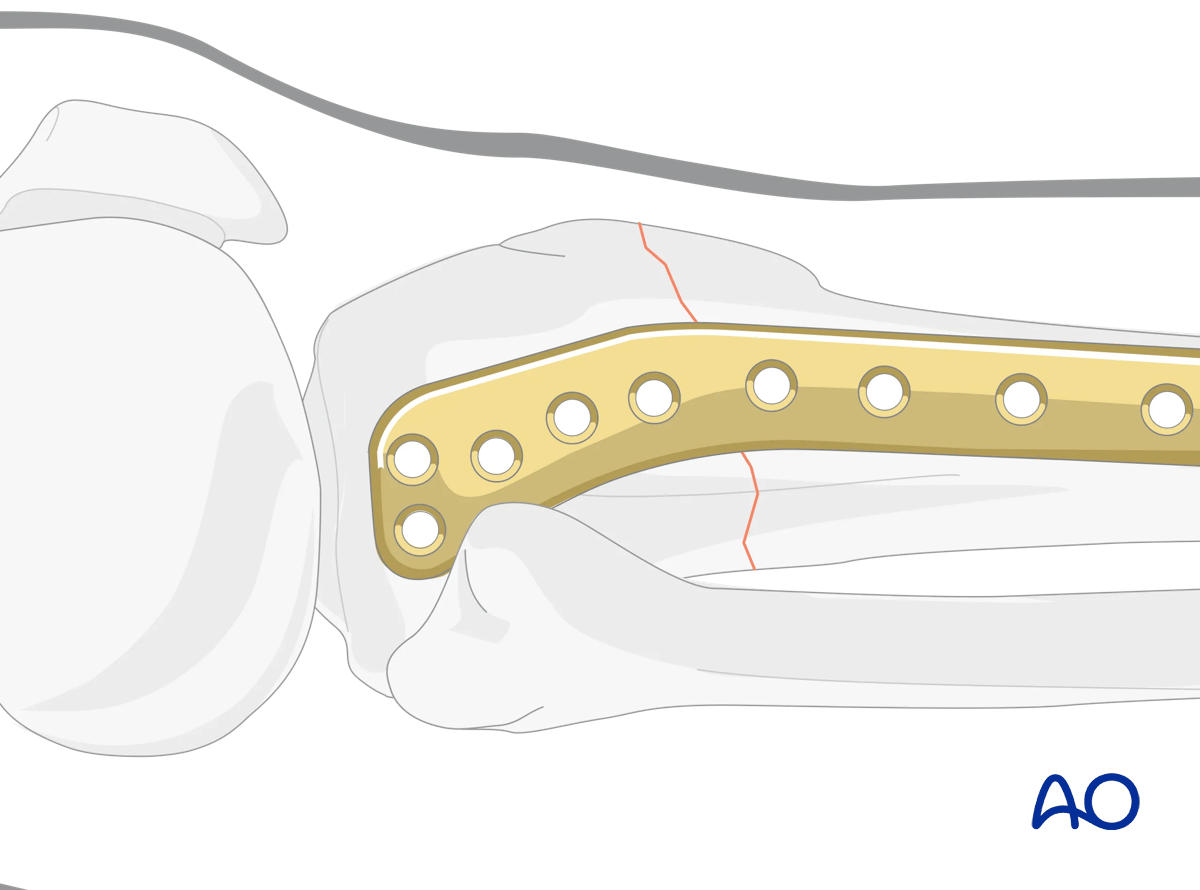
The plate should closely fit the proximal meta-epiphysis to minimize plate prominence.
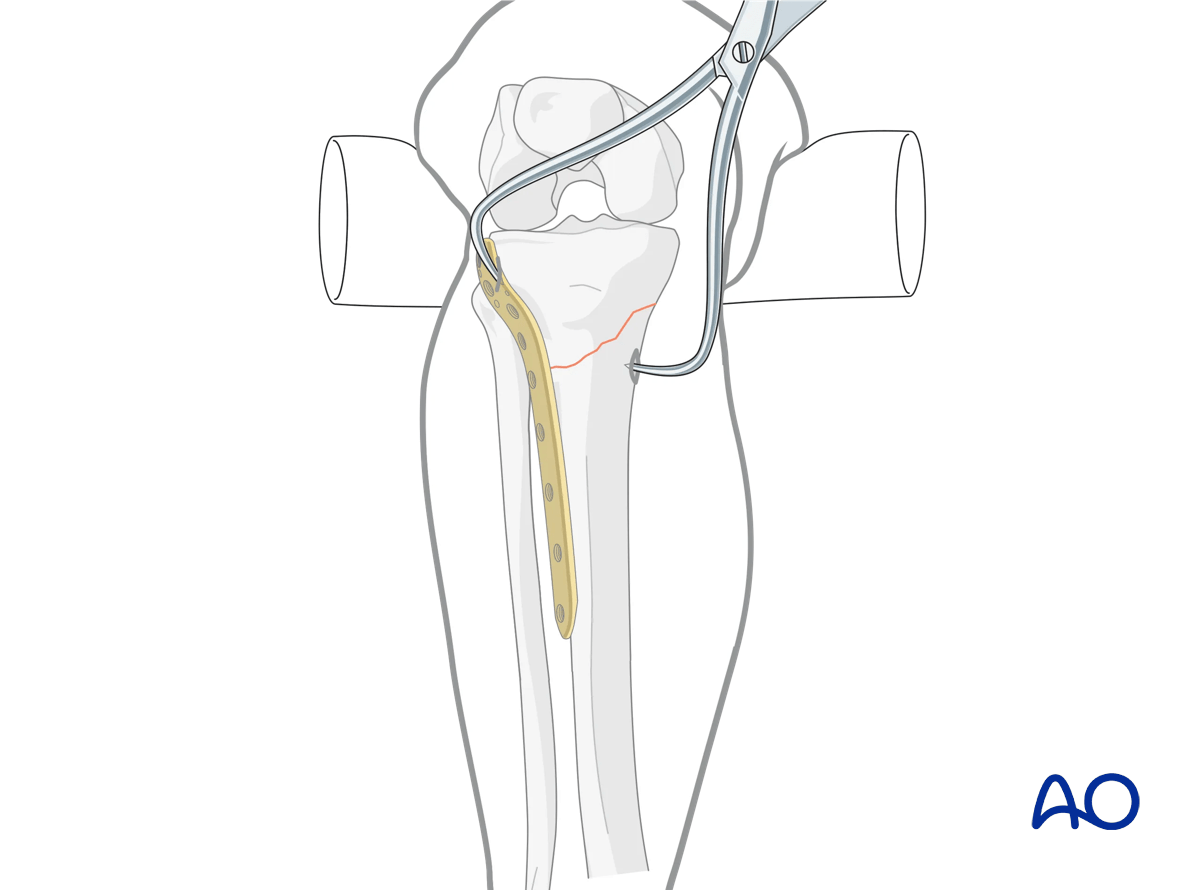
The appropriate position for the plate is immediately anterior to the fibula head.
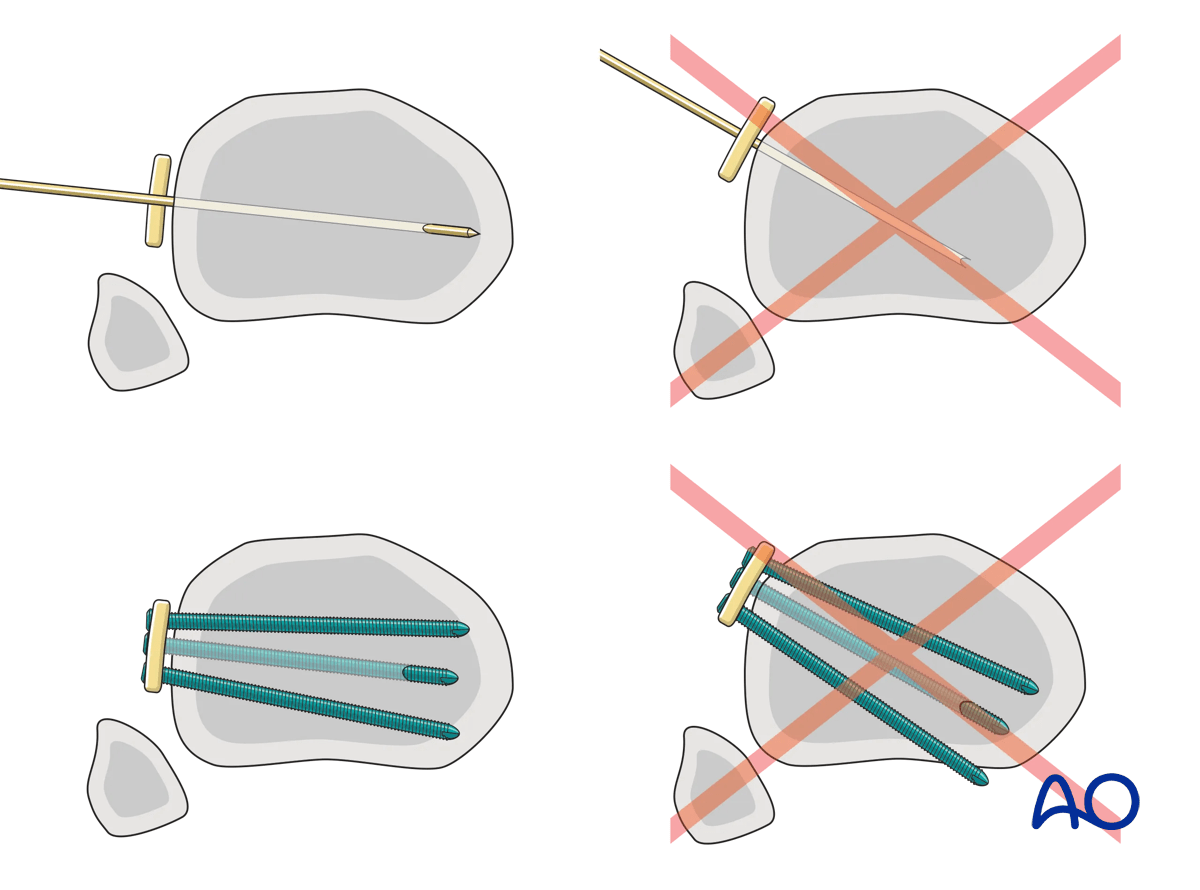
When inserting screws from lateral to medial the anatomy of the plateau must be taken into consideration in order to avoid penetrating the concave medial joint surface.
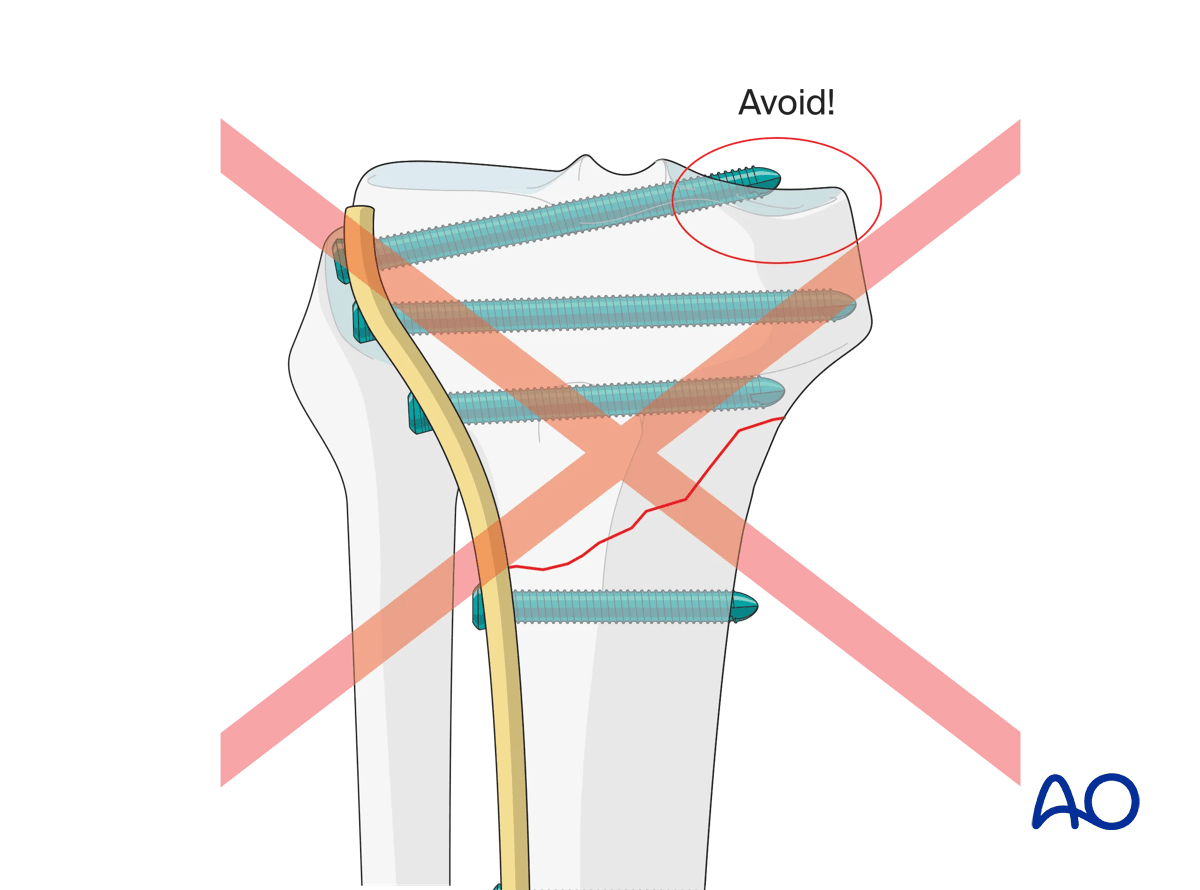
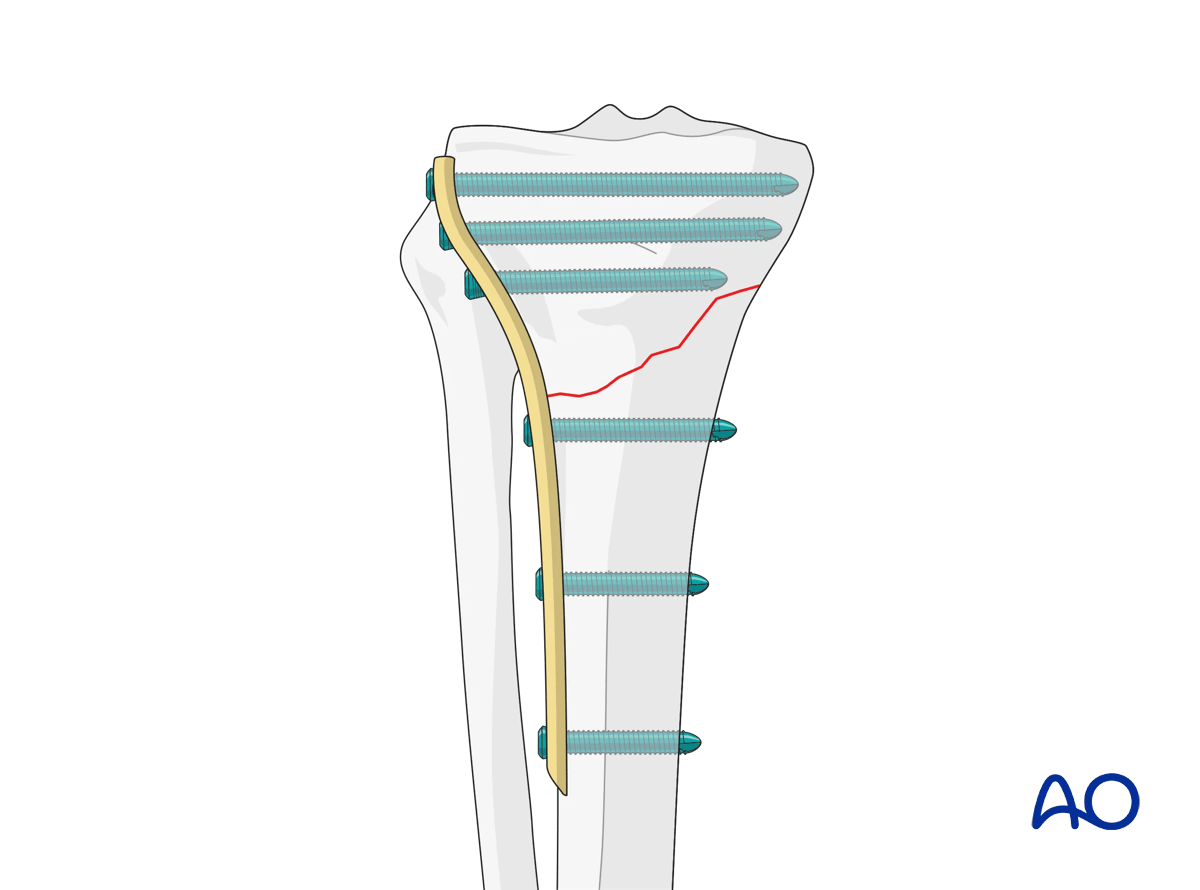
Plate location and rotation determine locking screw trajectory. Inadvertent internal rotation of the plate risks premature posterior extrusion and neurovascular compromise.
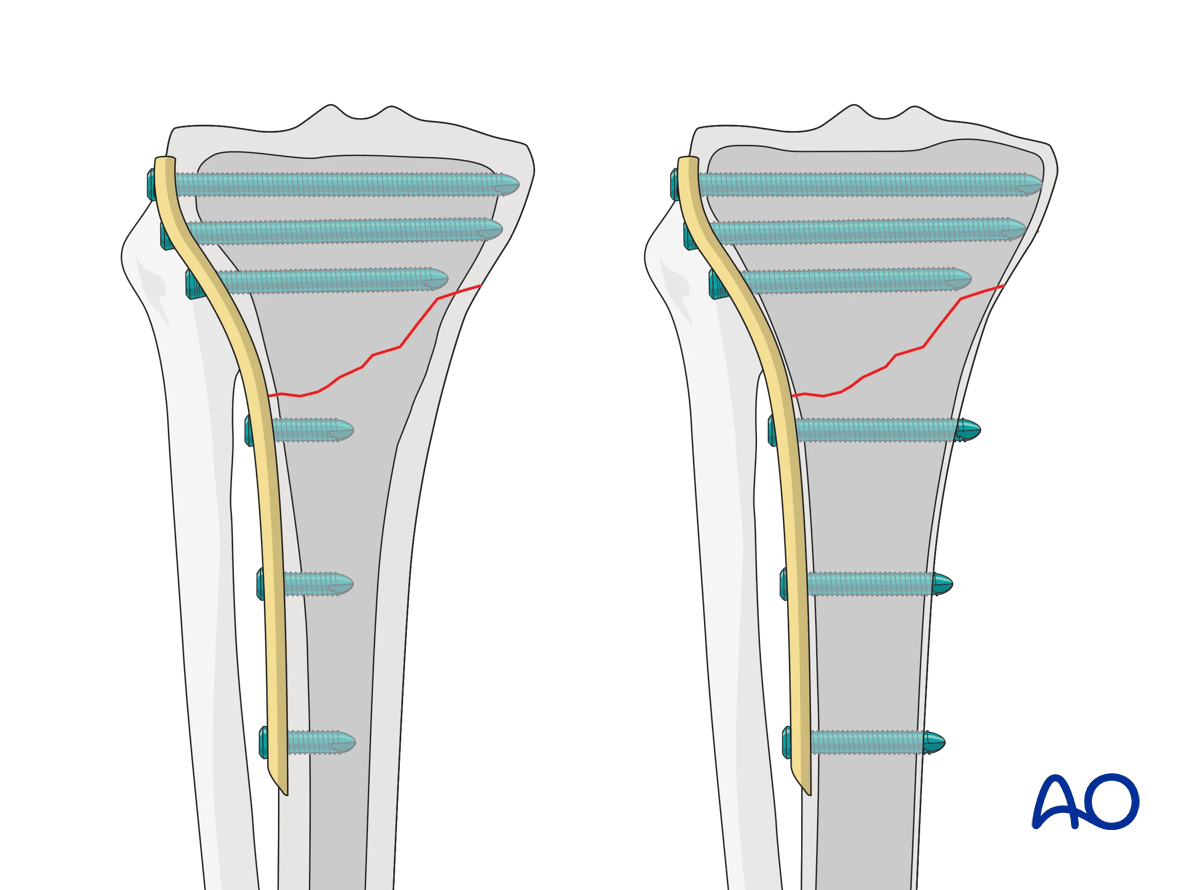
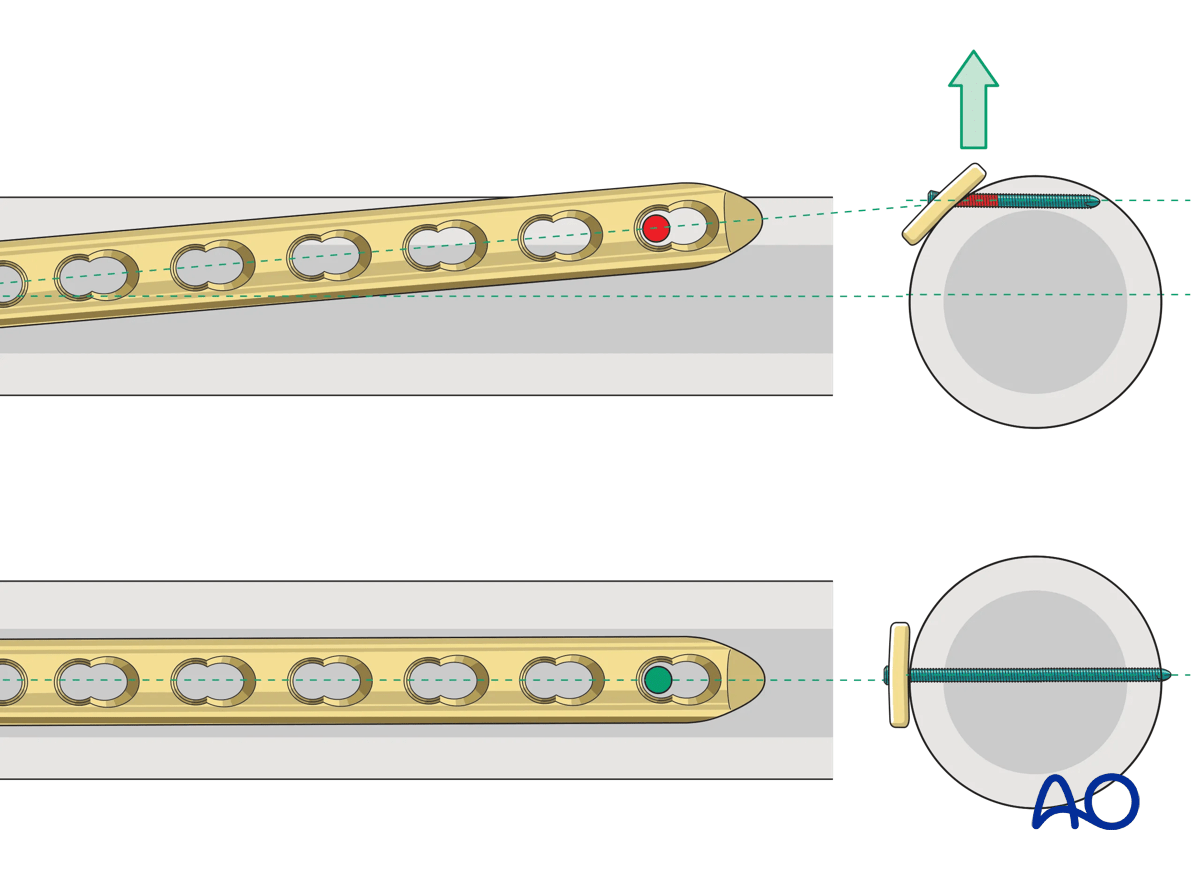
Distally, the trajectory of the screws should be into the medullary canal. This cross-section illustration shows incorrect and correct screw placement.
Appropriate plate fixation involves fixing the proximal plate to the bone with a single screw or K-wire in the correct position. This allows for sagittal plane correction. Then a fluoroscopic or clinical check is carried out to ensure that the distal plate is centered over the intramedullary canal. Once confirmed additional proximal and distal fixation is carried out, locking the position of the plate to the bone.
Wound closure
The wound should be closed with care taken to reapproximate the iliotibial band at Gerdy’s tubercle over the top of the plate. This will help minimize plate prominence.
7. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













