ORIF - Conventional plating
1. Principles
General considerations
Split depressed partial articular fractures of the lateral plateau are very common. Meniscal tears, articular incongruity, malalignment, condylar widening, and knee joint instability are all indications for surgical management. Significant soft-tissue injury is typically not associated with these injury patterns.
In order to illustrate the difficulties that may be encountered, we have included a full discussion under the respective sections.
Main steps in treatment include the following:
- Adequate preoperative planning (need for bone graft, approach(es), number and type of implants, sequence of reduction and fixation, additional equipment)
- Lateral sub-meniscular arthrotomy and joint distraction allow articular visualization and reduction
- Anatomical reduction of the articular surface with disimpaction of fracture fragments
- Bone grafting of the epiphyseal/metaphyseal defect once the fragments are disimpacted and the articular component elevated
- Definitive stable fixation performed with the buttress plate technique
Plate location
Plate location should allow for a raft of screws to be placed immediately below the elevated articular fragments. The plate length should travel distal to the exit point of the split fragment to reliably prevent caudal displacement of the lateral epiphyseal (split) fragment.
Potential complications
The following complications should be checked for during surgery:
- Articular malreduction
- Alignment malreduction
- Intraarticular hardware
- Prominent fixation
- Unlike the C type injuries and medial B type injuries vascular and nerve injury and compartment syndrome are very unusual
2. Preparation
Patient positioning
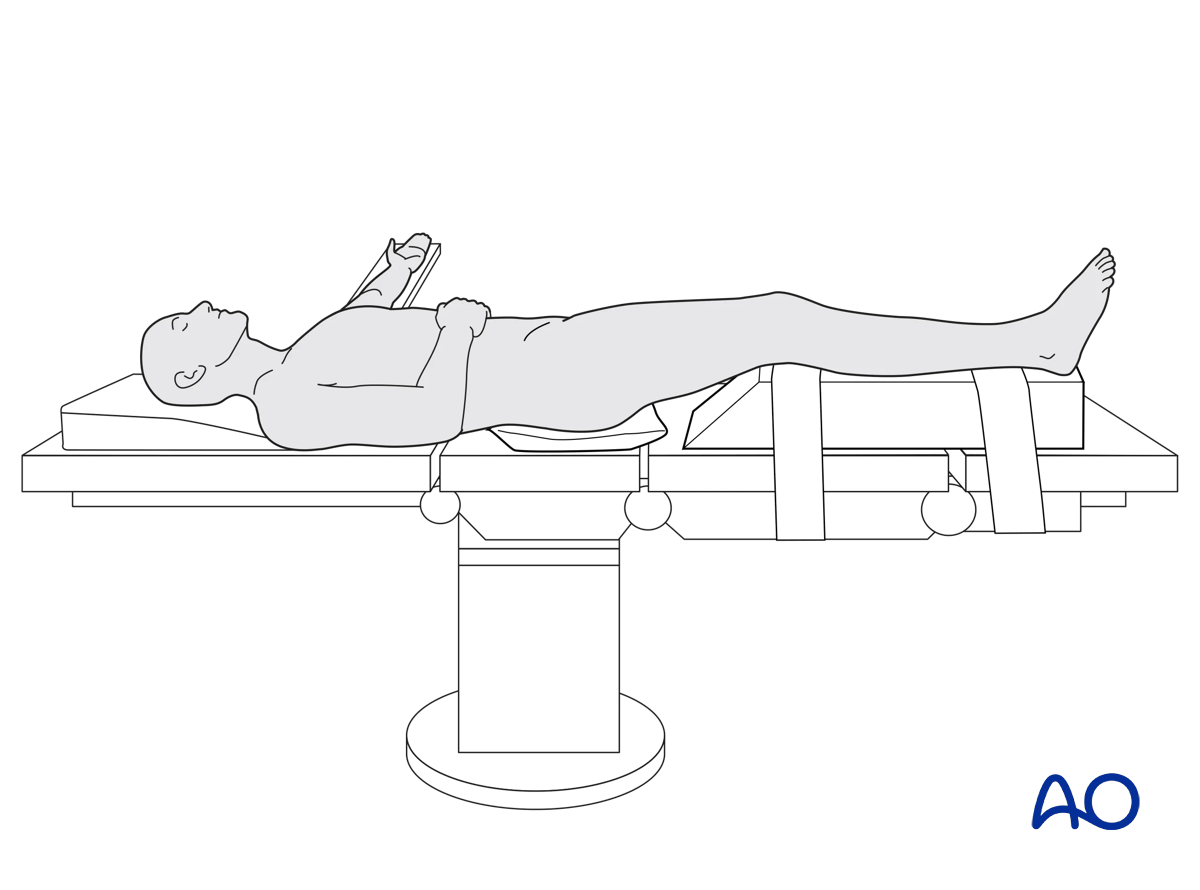
The patient is placed in the Supine position.
A tourniquet is helpful in most cases. Whether a tourniquet is used depends on the amount of bleeding. Exsanguinate the limb by elevating it.
To allow for intraoperative radiographic control of reduction and fixation, the use of a radiolucent table is mandatory.
The vast majority of subarticular and metaphyseal bone defects are currently filled with morcellized cancellous allograft and/or bone graft substitutes. These should be available during the procedure. Autologous bone graft is rarely utilized.
3. Approaches
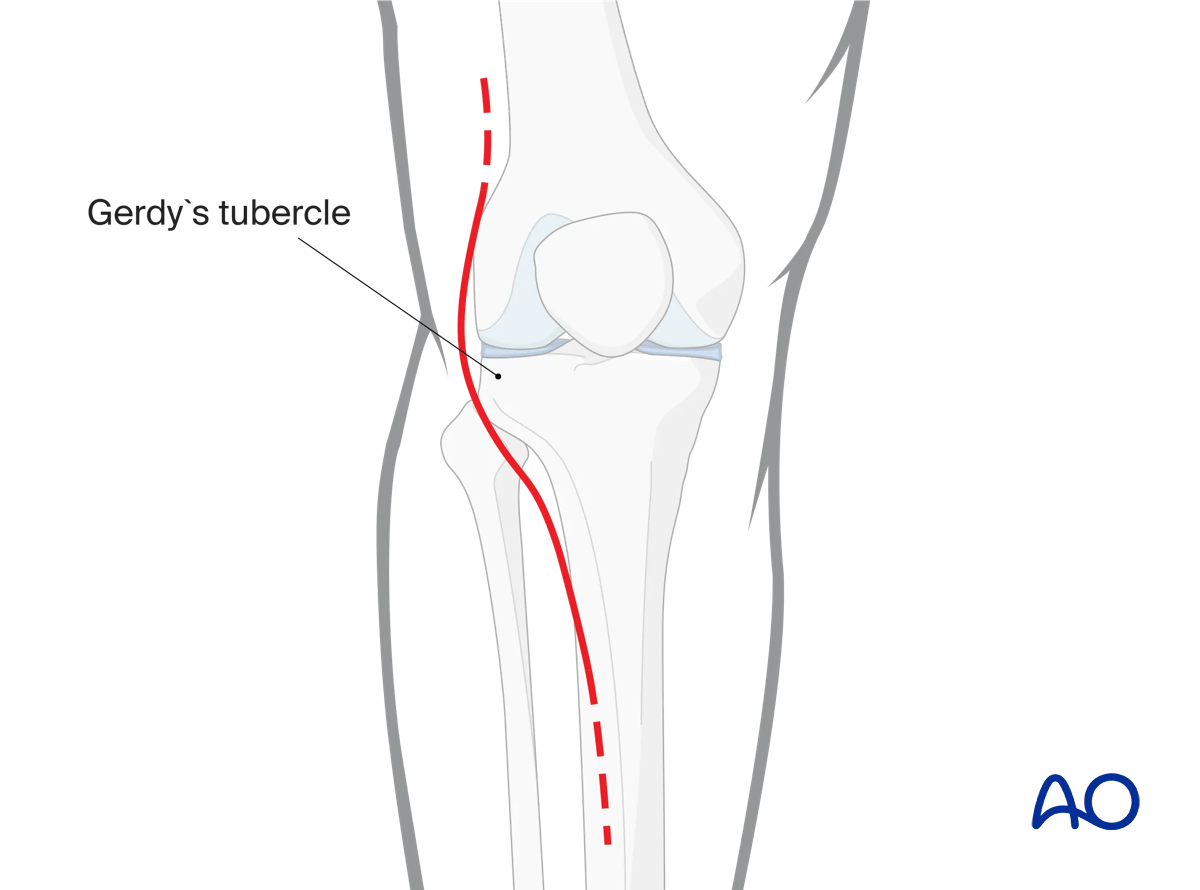
An anterolateral approach is used for the vast majority of cases. If a greater visualization posteriorly is required, the extended anterolateral approach can be utilized.
4. Preliminary reduction
General considerations
Contralateral imaging of the other knee will help determine the final height of the articular surface and frontal and sagittal plane alignment.
The injured knee should be examined under anesthesia and a sense of frontal plane instability to valgus force can be identified.
Ligamentotaxis will not reduce depressed articular fracture fragments. Direct elevation, with the use of bone tamps and dental picks, is required.
Reduction of the lateral articular surface
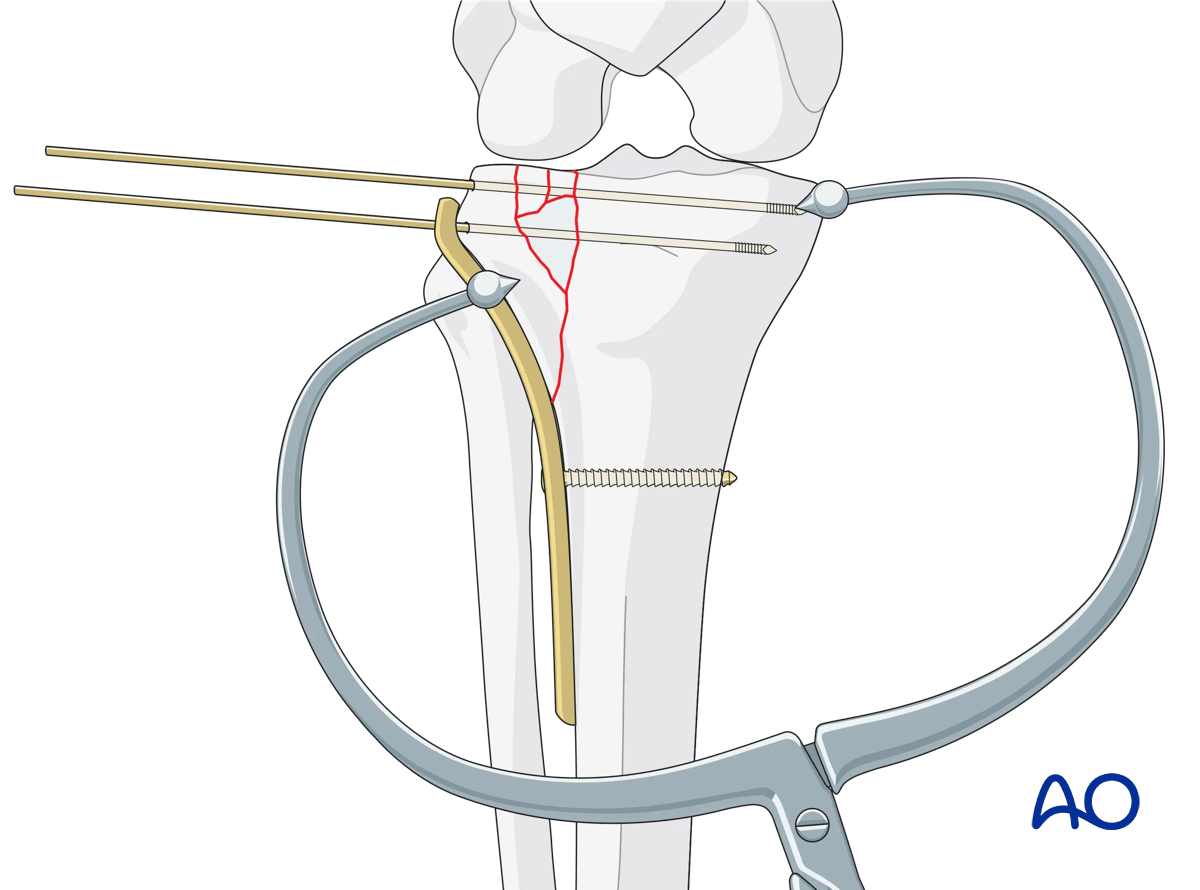
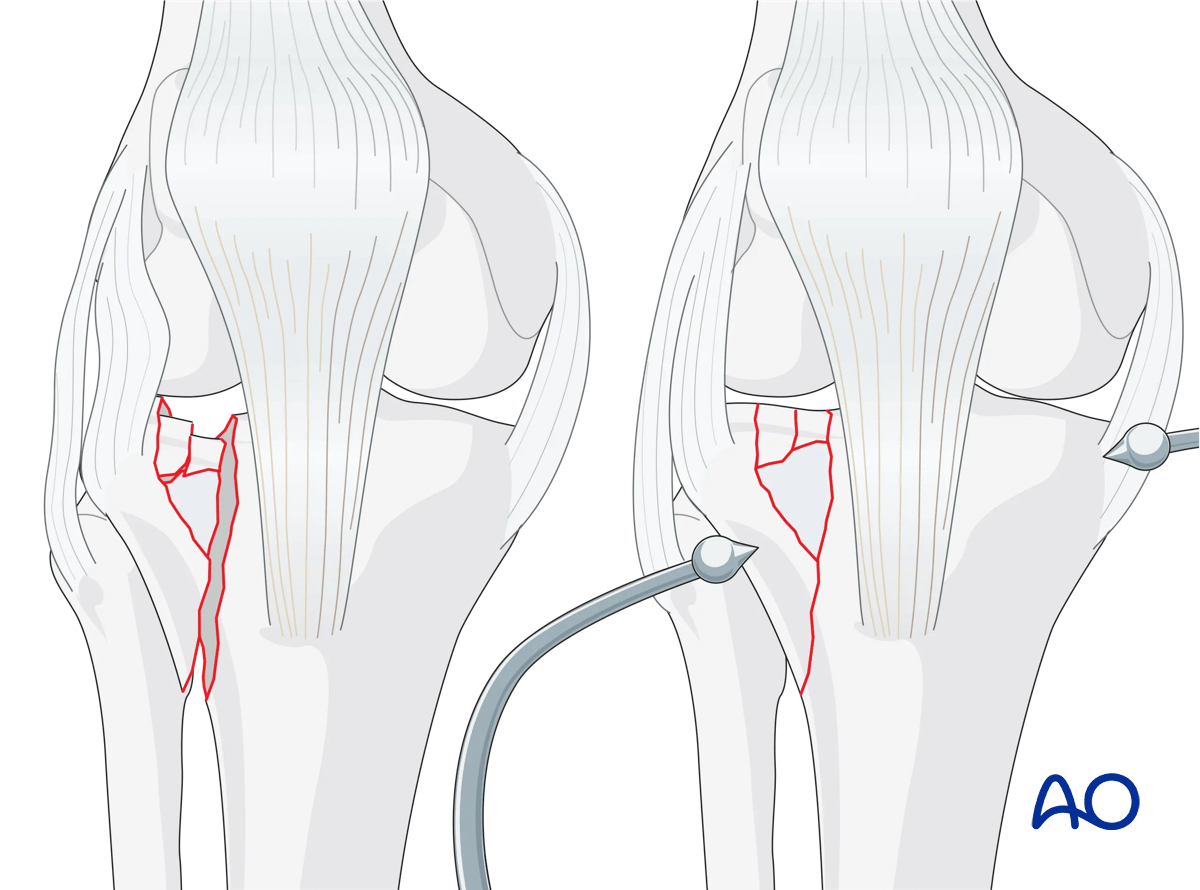
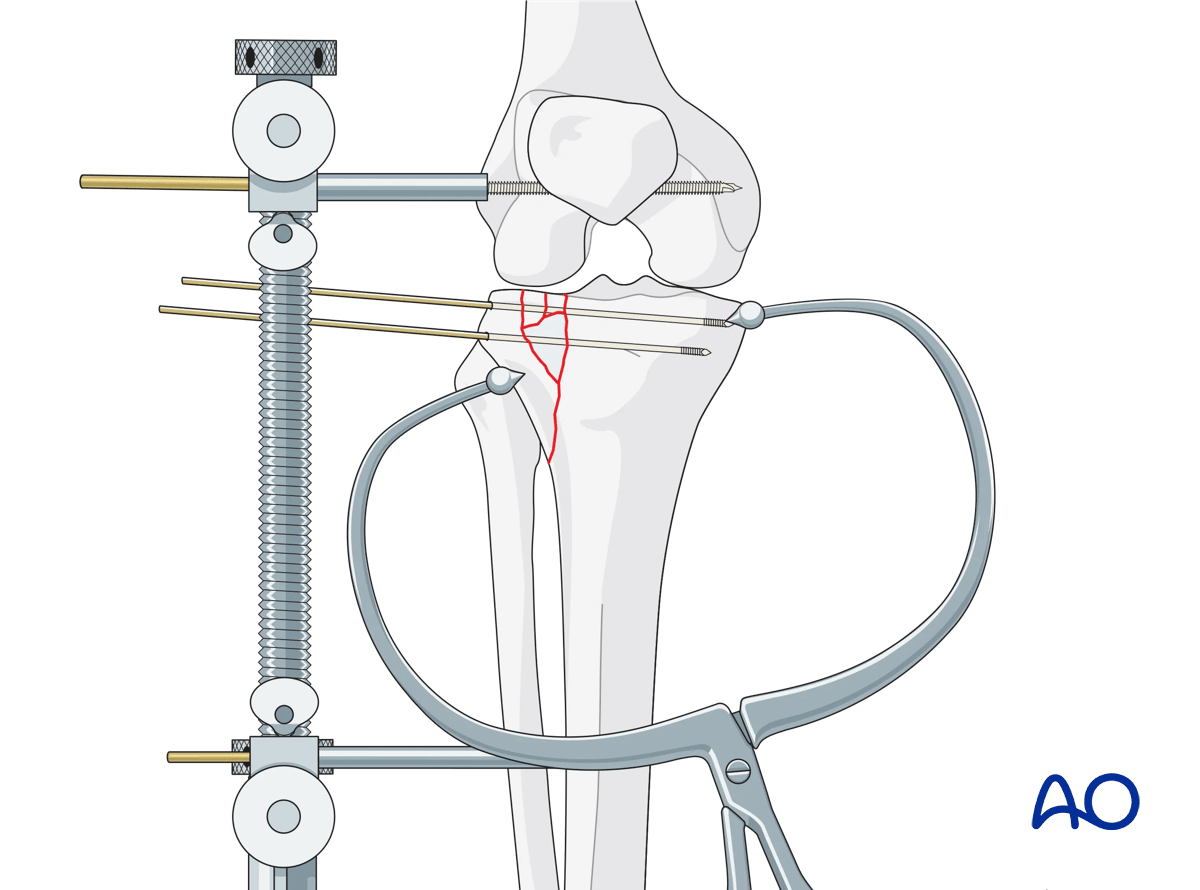
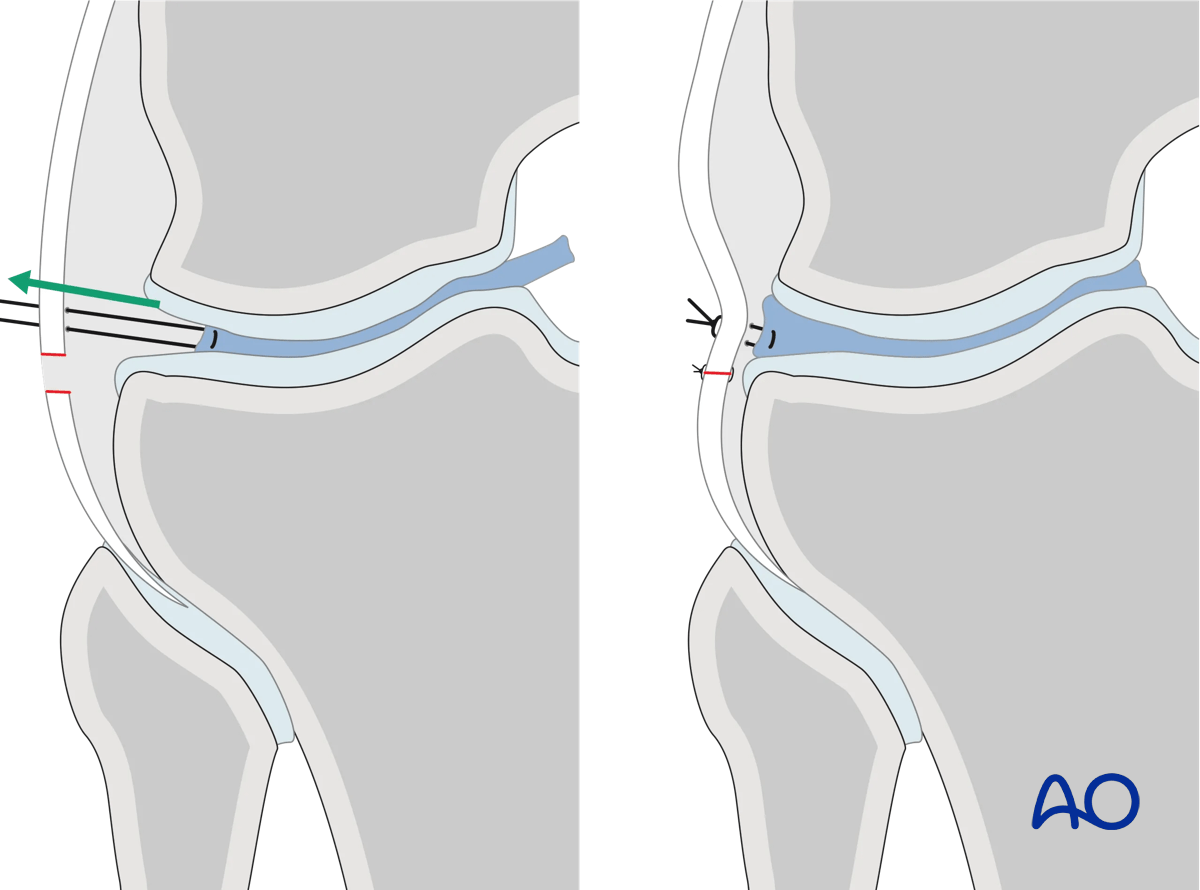
Containment technique (preferred)The lateral articular and cortical surfaces are exposed using the anterolateral approach. Cleansing of the cancellous surface hematoma and clearing periosteum from the cortical surface of the split fracture fragment margins is performed. The lateral cortex is reduced using cortical interdigitations as a guide for an accurate reduction. The split fracture is now stabilized with K-wires and clamps. Reduction of the depressed lateral articular surface now requires careful joint visualization. A laterally-based femoral distractor is used, and careful distraction is then applied. A sub-meniscal arthrotomy is performed once the joint has been distracted. At this point the lateral meniscus should be identified and found to be attached to the peripheral capsule. It is not uncommon for the peripheral meniscus, however, to be partially or completely detached from the capsule. In situations with complete detachment, the meniscus may be identified more centrally within the lateral compartment, trapped along the articular fracture line, or resting on top of the depressed articular fragments.
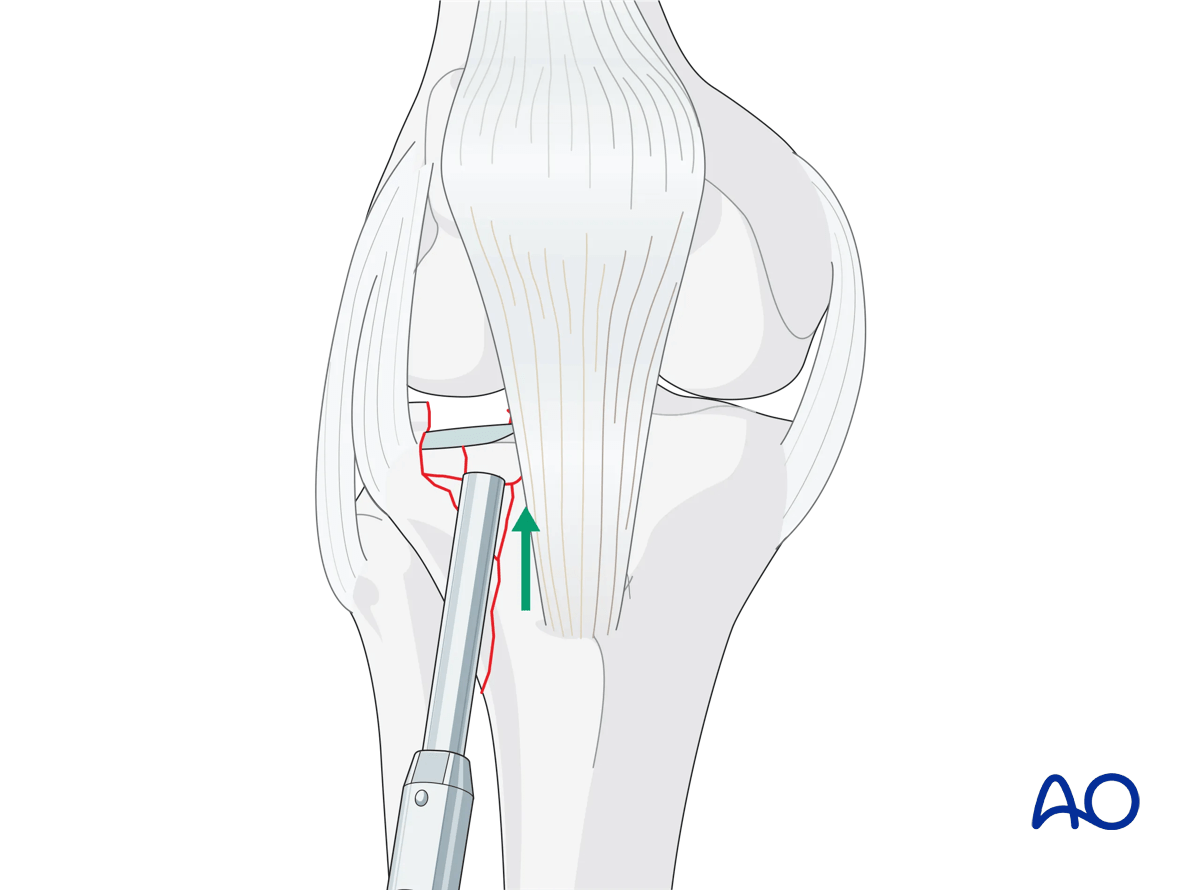
A cortical window is then created through the reduced split fragment, and a bone tamp is used to elevate the depressed articular fragments. Accurate reduction is identified with direct visualization and radiographic confirmation.
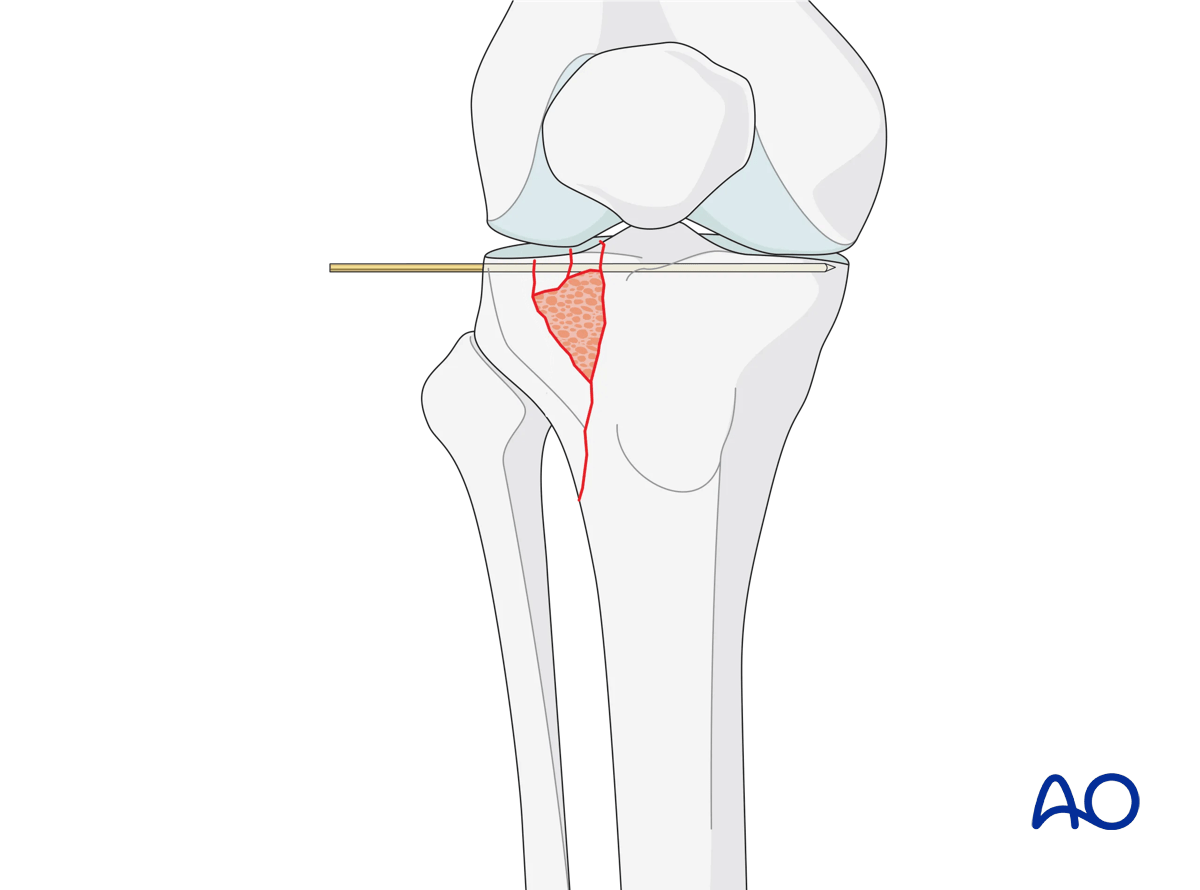
Subchondral K-wires are used to maintain the reduction, and the bone defect is grafted. At this point, the articular surface should be reduced, and the frontal and sagittal plane alignment should be closely evaluated.
The split fragment and articular reductions may be compressed by adjusting the clamp. Anatomic articular reduction is prioritized over the cortical interdigitations. Accurate reduction is confirmed radiographically, and with direct visualization.
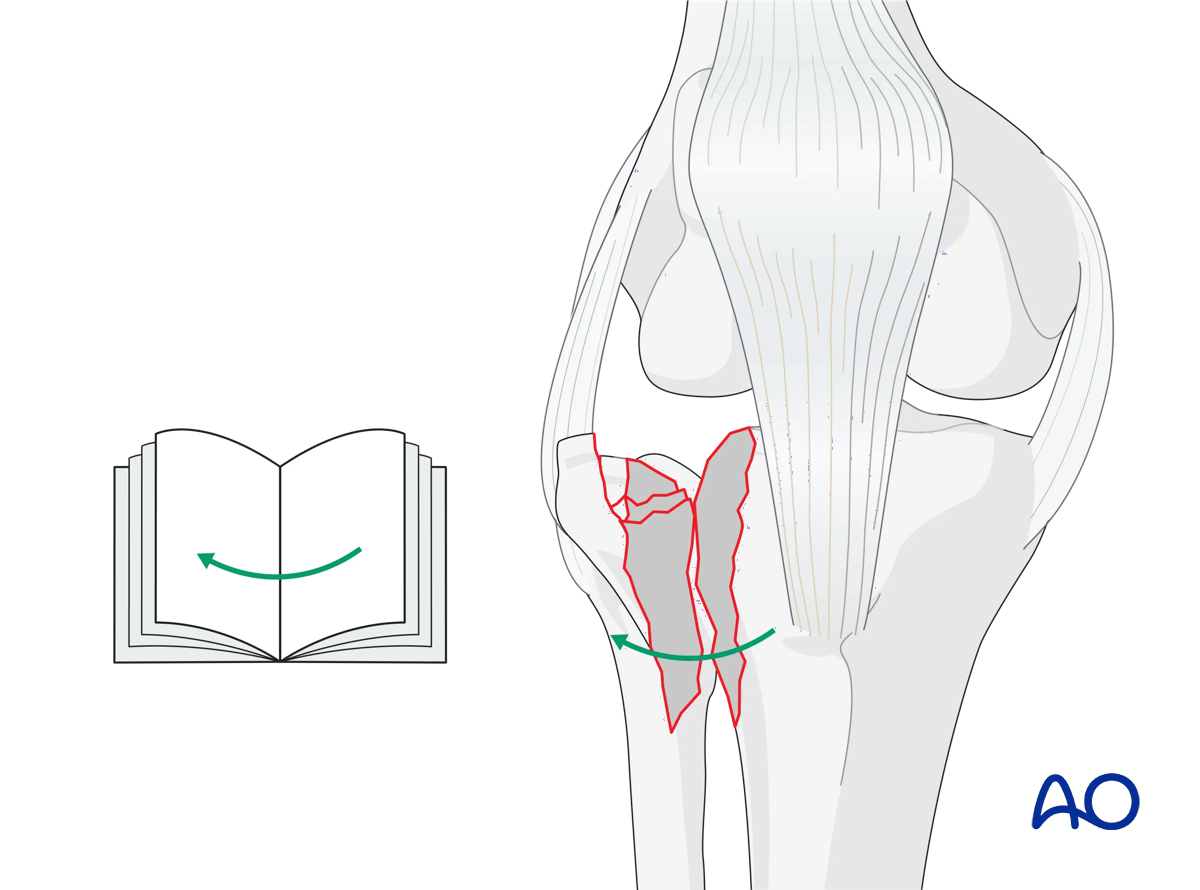
In the open book technique, the split fragment is not reduced initially, but opened, much like a book, exposing the cancellous surfaces enabling visualization of the depressed articular fragments from the front. After joint distraction the articular fragments are now elevated and reduced by working within the cancellous surfaces of the main fracture fragments. As in the containment technique, once the depressed articular fragments are elevated to the intact tibia, K-wires are used to maintain their position. Bone graft may be inserted at this point, and then the split component is reduced. The articular surface is visualized and adjusted as needed. The open book technique is useful when there is a single large depressed articular segment that is markedly angulated or markedly depressed.
In the majority of cases the containment technique is preferred.
Fixation of the lateral column
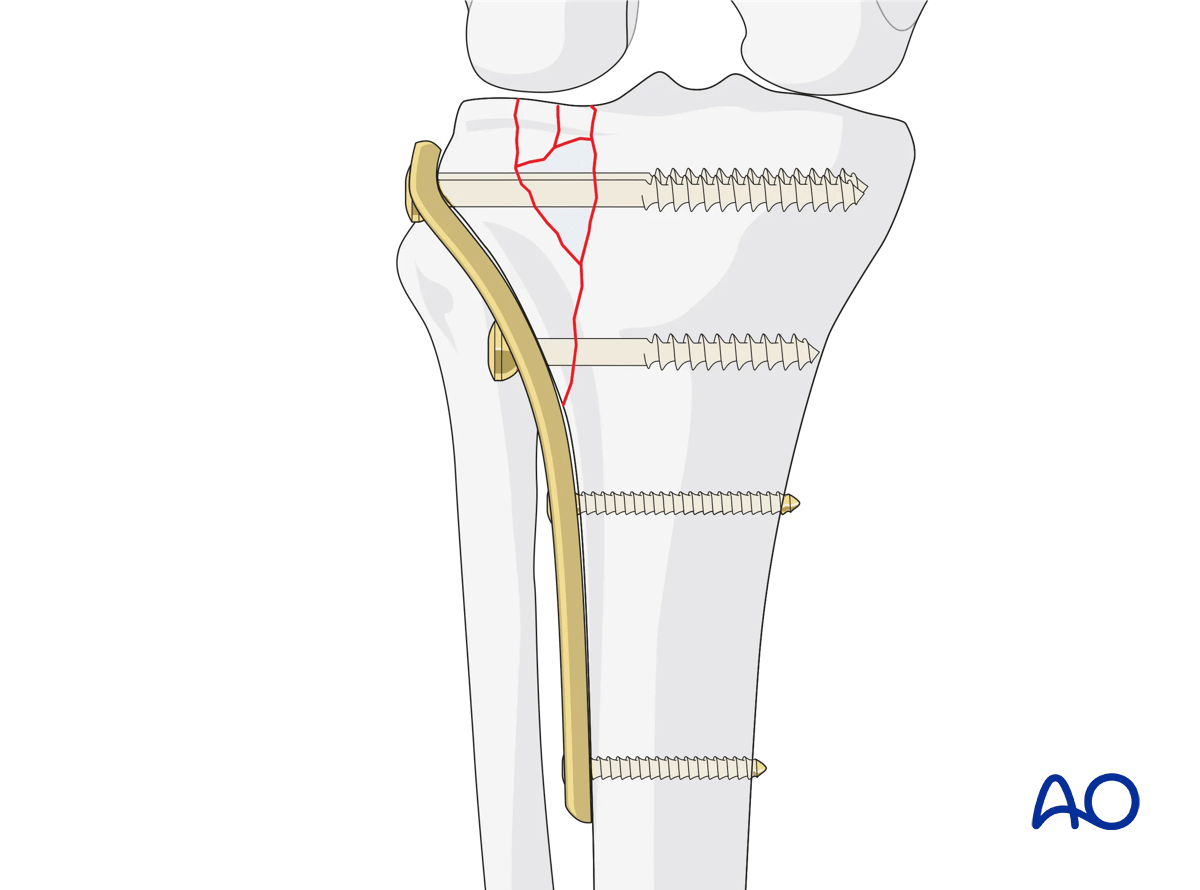
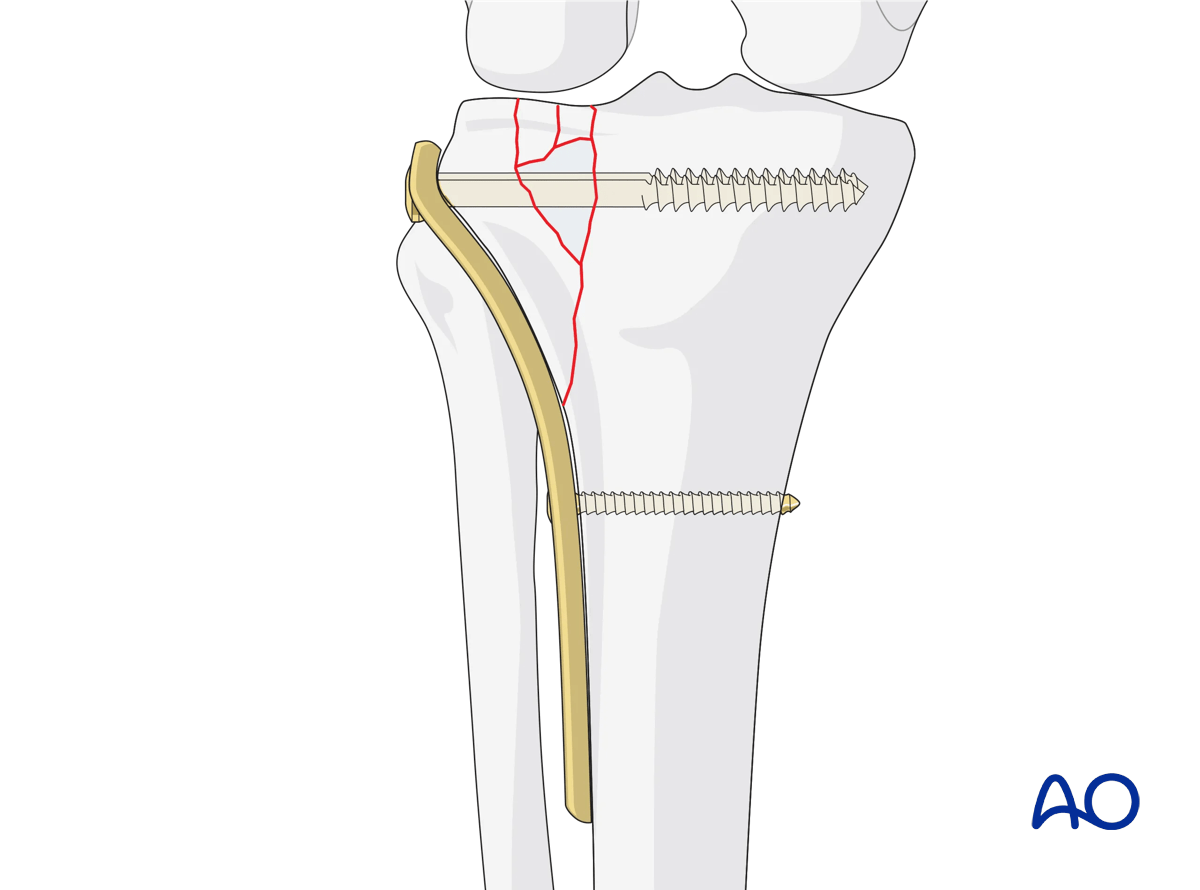
The lateral column is stabilized with traditional buttress plate fixation. Plate length should allow for adequate fixation distal to the exit point of the split fragment. Periarticular plates contoured to the proximal lateral tibial plateau are the preferred implant. Fixation begins in the metadiaphyseal region immediately distal to the exit point of the split component. This traps the split component, resisting its distal displacement. Fixation then proceeds proximally, with the use of lag screws through the plate to compress the split fragment to the remaining proximal tibia. Conventional screw-plate devices will compress the plate to the lateral cortex and create interfragmentary compression. A raft of screws from lateral to medial through the proximal portion of the plate will function to support the elevated lateral articular surface. Care should be taken to ensure that the plate is placed proximally enough to allow the proximal screws to support the elevated articular surface.
Final osteosynthesis
Once osteosynthesis is completed, make a final check with the image intensifier. If all is well, remove the femoral distractor. The knee should then be placed through a full range of motion to ensure fracture stability, and frontal-plane stability in full knee extension can be reexamined. At this point the knee should demonstrate improved stability to valgus force.
In situations with meniscal disruption from the capsule the meniscus can be repaired back to the capsule using absorbable mattress sutures. The submeniscal arthrotomy is then closed, ideally with a watertight closure. In situations where the capsule is deficient from the lateral proximal tibia the capsulotomy can be repaired to the proximal portion of the lateral plate.
Closure
The ilio-tibial band is then closed over the top of the lateral tibia plateau plate. Distal to Gerdy’s tubercle the anterior compartment fascia can be closed if there is no concern for significant postoperative swelling. In situations where there is significant concern, the surgeon has two options:
- Closure of the anterior compartment fascia with a subsequent anterior compartment fasciotomy performed lateral to the fasciotomy for surgical exposure.
- Leaving the anterior compartment fascia open. This option has a potential risk of leaving only skin and subcutaneous tissue closed over the internal fixation.
Dermal suture is used sparingly to reapproximate the skin. The skin is then closed with interrupted vertical mattress nylon suture or Allgower-Donatti suture. If not, the fascia may be closed.
5. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













