Screw fixation
1. Principles
General considerations
Avulsion of the posterior cruciate ligament is unusual and may occur in isolation or in more complex fracture dislocation patterns. A clinical assessment of associated ligamentous injury and knee stability should be performed. Neurovascular injury may also be present as the risk is similar to that of a knee dislocation. Fixation of a posterior cruciate avulsion injury can markedly improve sagittal plane knee stability and is worthwhile. Associated posteromedial articular injury may occur, as well as posterolateral corner injuries.
Timing of surgery
Surgery should be performed when soft tissue, patient, and operating conditions are satisfactory.
Prior to surgery, the limb should be immobilized (eg, with an external fixator, knee immobilizer, splint, etc).
Potential complications
The following complications should be checked for during surgery:
- Fragment malreduction
- Intraarticular hardware
- Prominent fixation (anteriorly)
- Vascular and nerve injury and compartment syndrome
2. Preparation
Patient positioning
The patient is placed in the prone position.
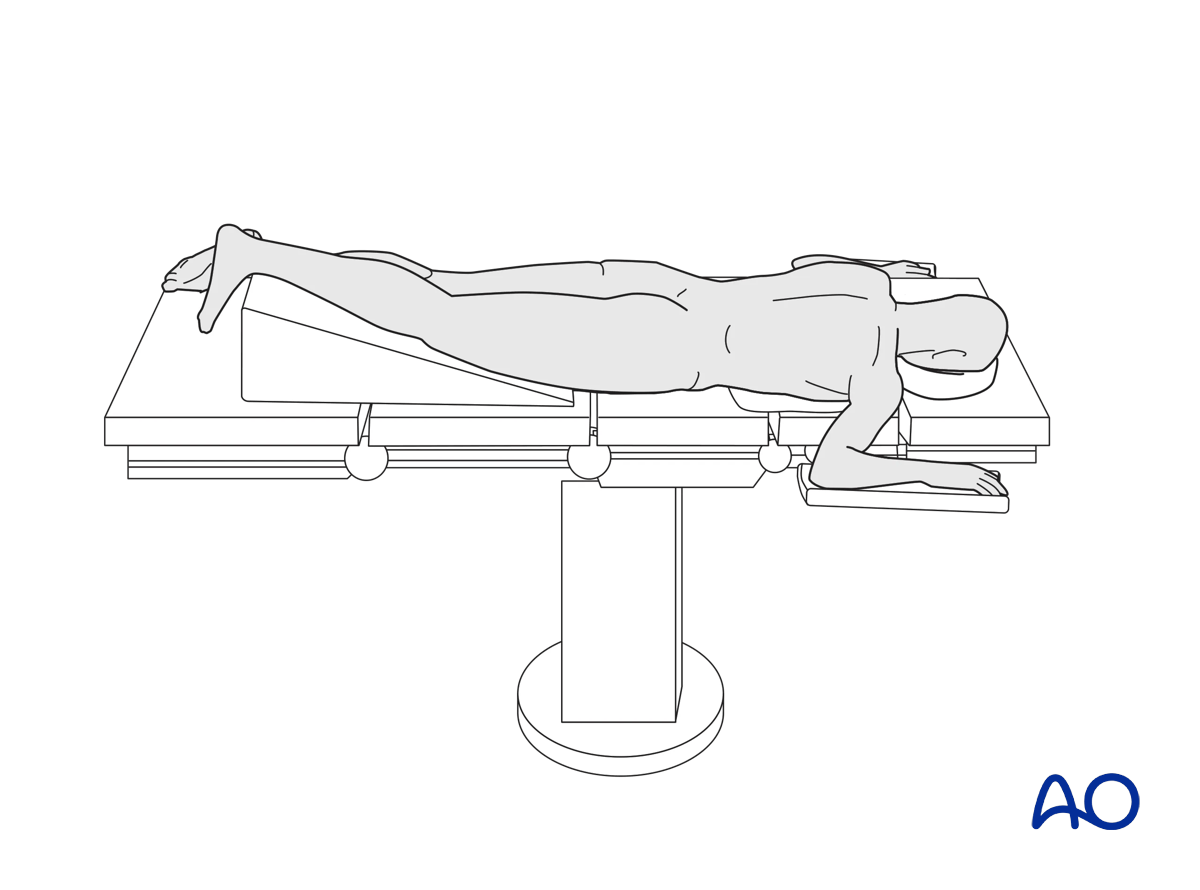
A tourniquet may be helpful.
To allow for intraoperative radiographic control of reduction and fixation, the use of a radiolucent table is mandatory.
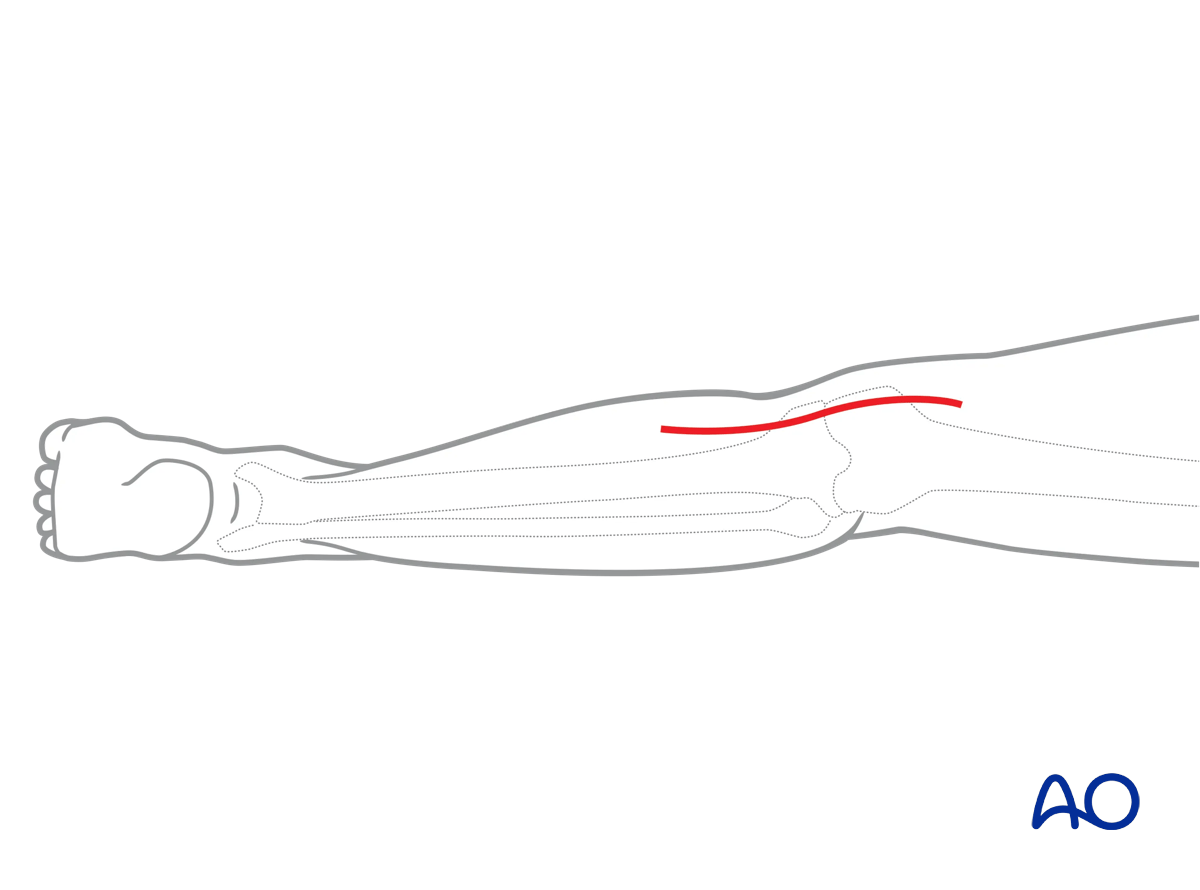
3. Approach
A posteromedial approach is used.
4. Preliminary reduction
General considerations
Contralateral imaging of the other knee will help determine the final height of the articular surface and frontal and sagittal plane alignment.
The injured knee should be examined under anesthesia and a sense of frontal and sagittal plane instability should be identified.
Ligamentotaxis will improve the reduction, but direct fragment visualization and reduction is preferred.
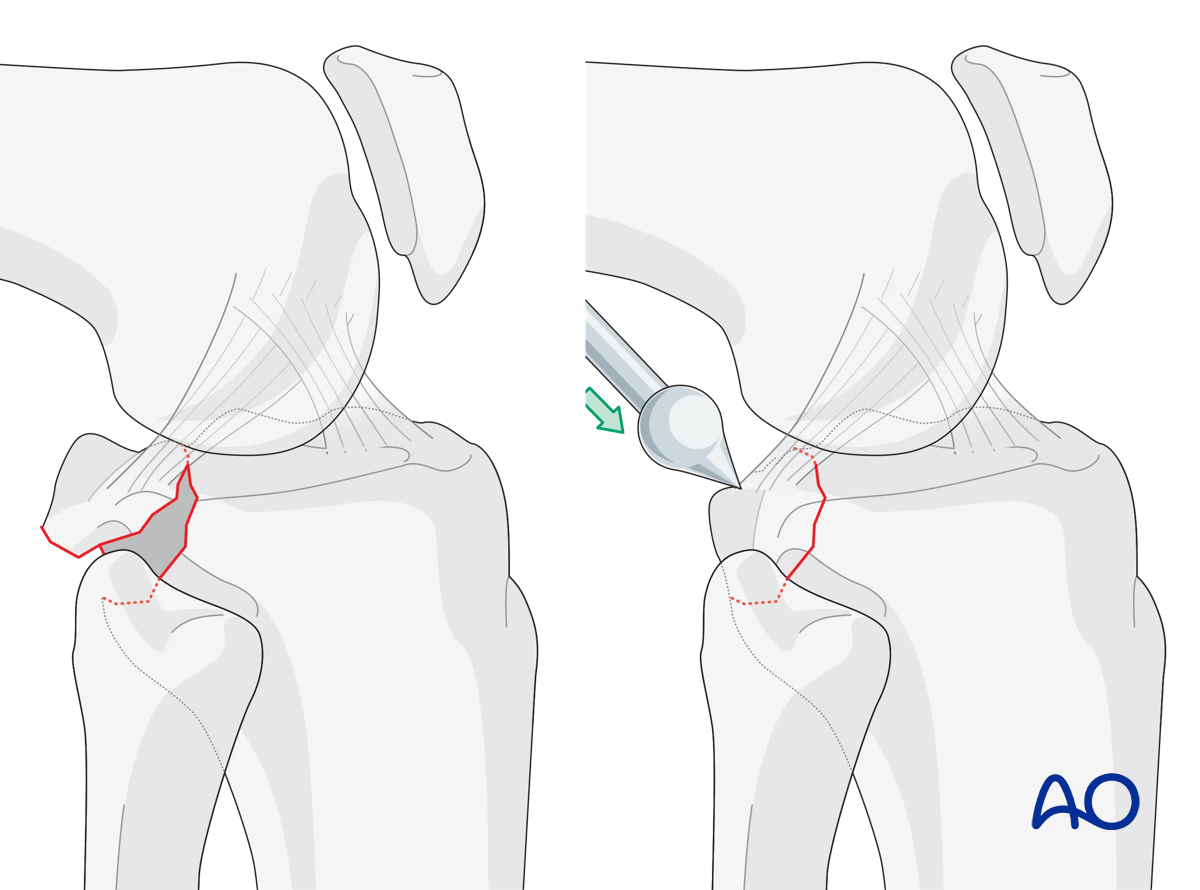
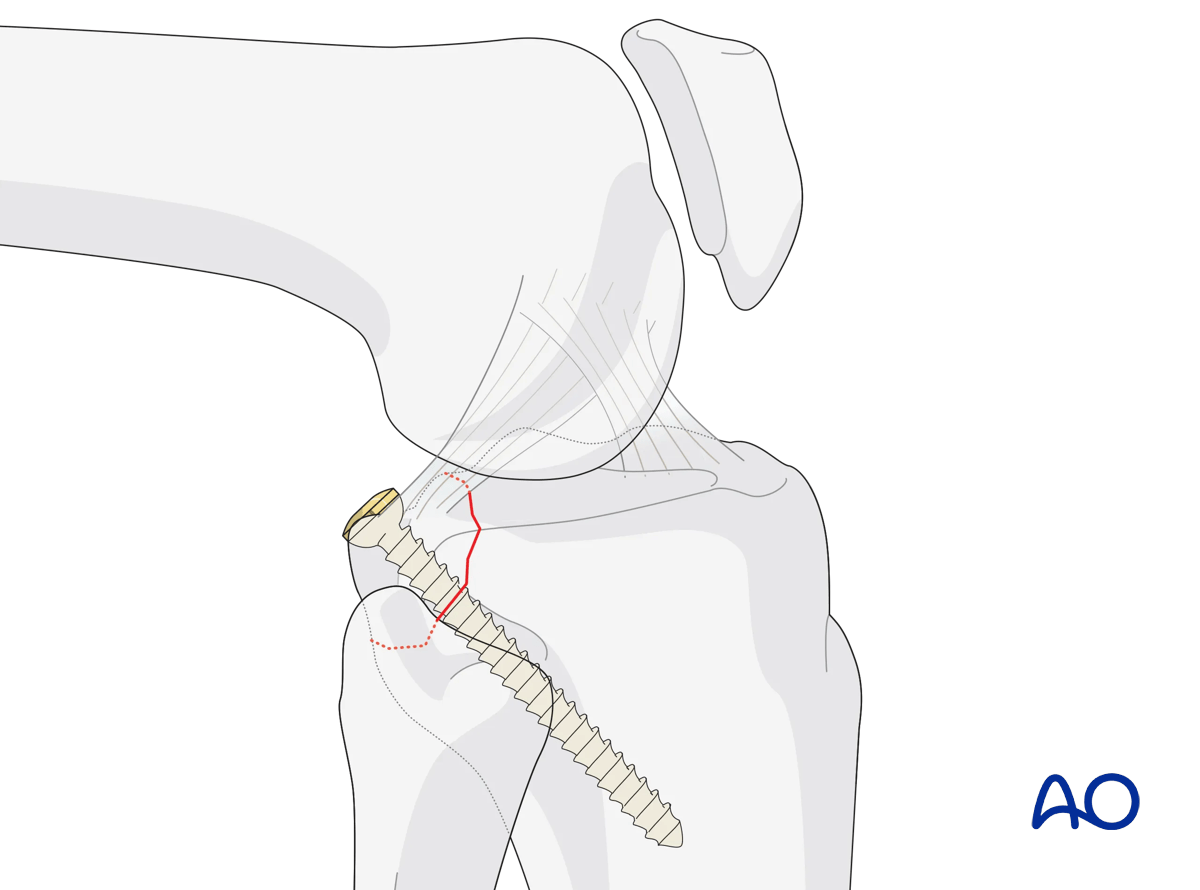
In many instances a very clear cancellous bed is identified that allows a direct reduction of the avulsed posterior cortex. This fracture surface should be cleansed, and the posterior cruciate ligament and its avulsed fragment of bone should be reduced and interdigitated. K-wires may be used to provisionally hold the reduction. A C-arm should be used to corroborate the reduction. Fixation can then occur with posterior to anterior lag screws under C-arm guidance. One or two small fragment screws are typically all that is necessary. In situations where the fragment is thin or comminuted, a washer or a low-profile malleable tubular plate may be used to improve fixation.
5. Closure
The wound is closed in layers.
6. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













