Prone posteromedial approach to the proximal tibia
1. Principles
The prone posteromedial approach has several advantages as compared to the same approach in the supine position. Lateral retraction of the medial gastrocnemius muscle is increased and easier. Access to the direct posterior metaphysis and posterior central parts of the epiphysis are facilitated. Commonly, with the knee in extension, reduction of the posteromedial fracture fragment is easier to achieve. Last, placement of implants, including drilling and measuring, is much simpler.
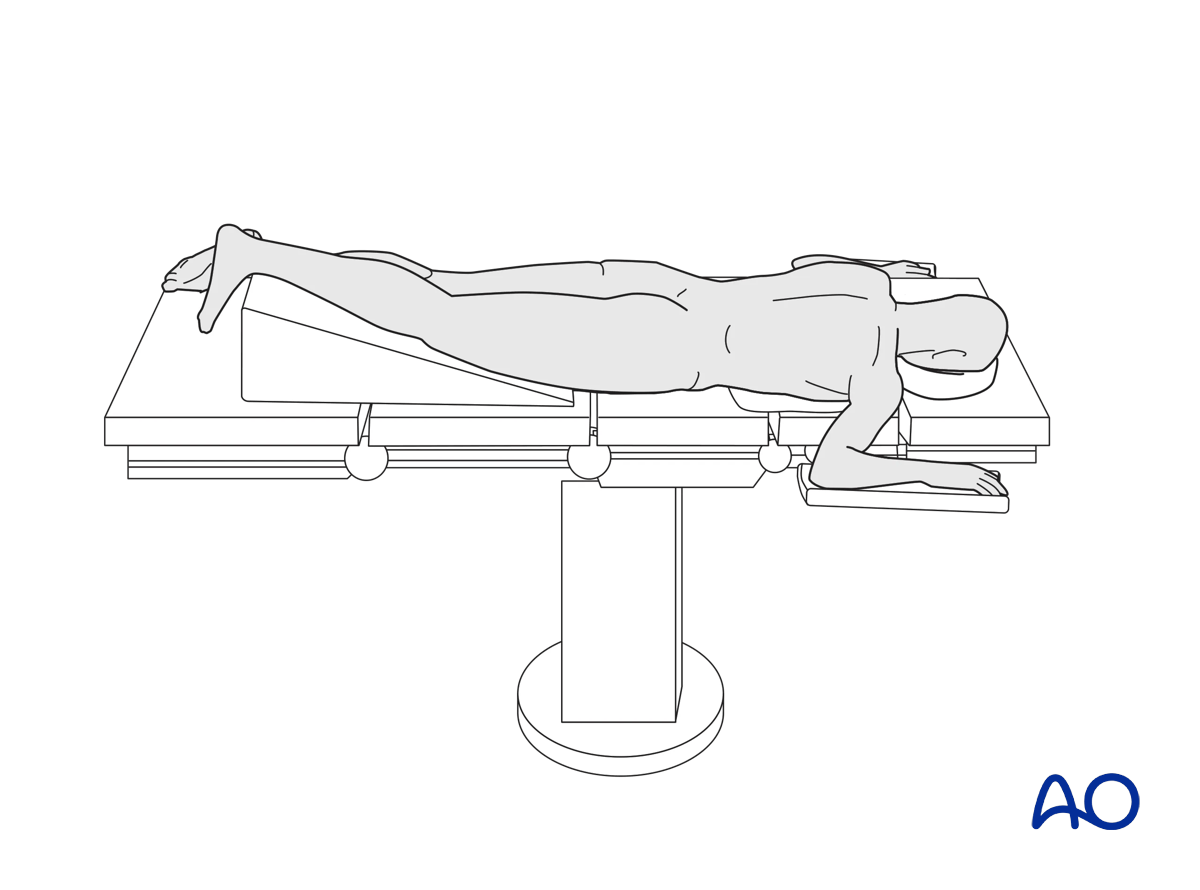
2. Patient positioning
The patient is positioned in a prone position.
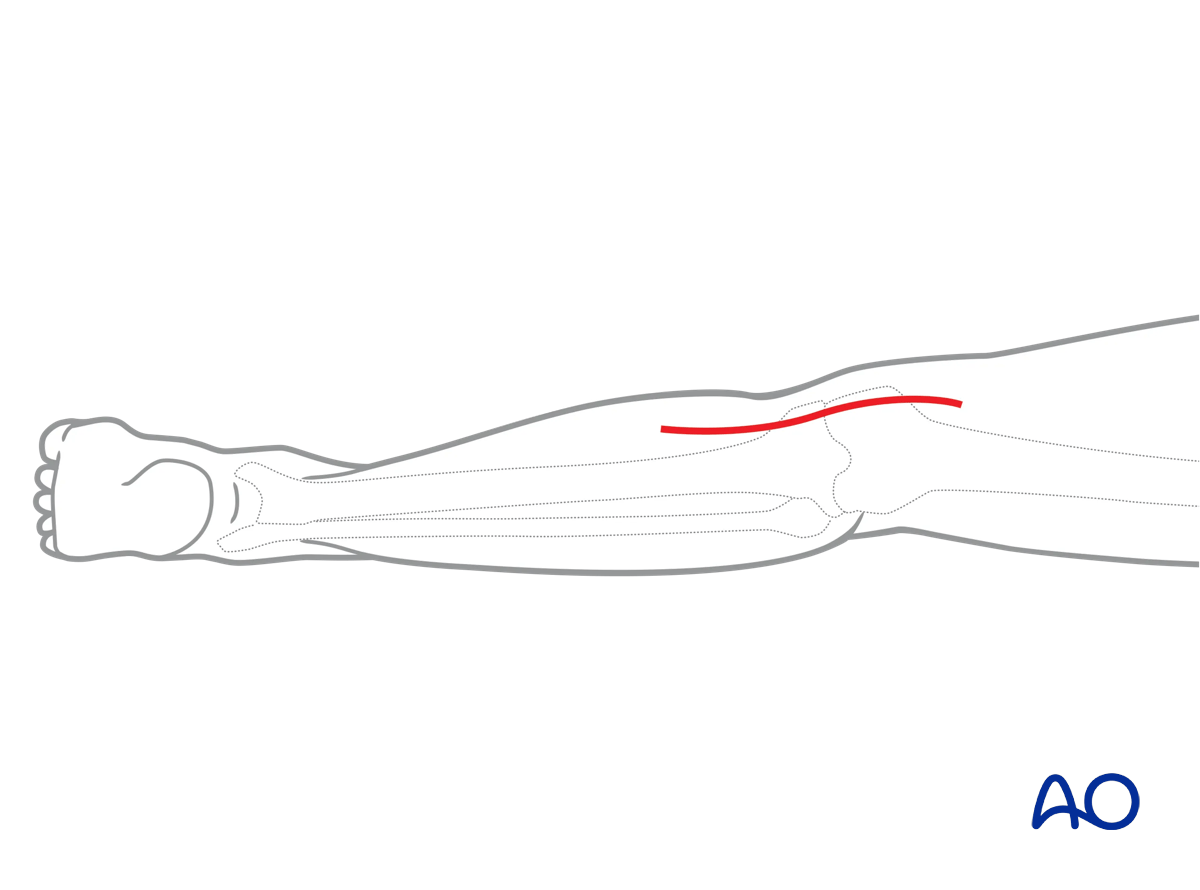
3. Skin incision
With the patient positioned an AP image intensifier view is used to identify the medial tibial cortex. Beginning distally and moving proximally, the skin incision will be placed longitudinally along this radiographic line. When the popliteal skin crease is encountered both lazy S and straight longitudinal incisions are acceptable.
Open the fascia over the medial head of the gastrocnemius muscle in line with the skin incision.
4. Deep dissection
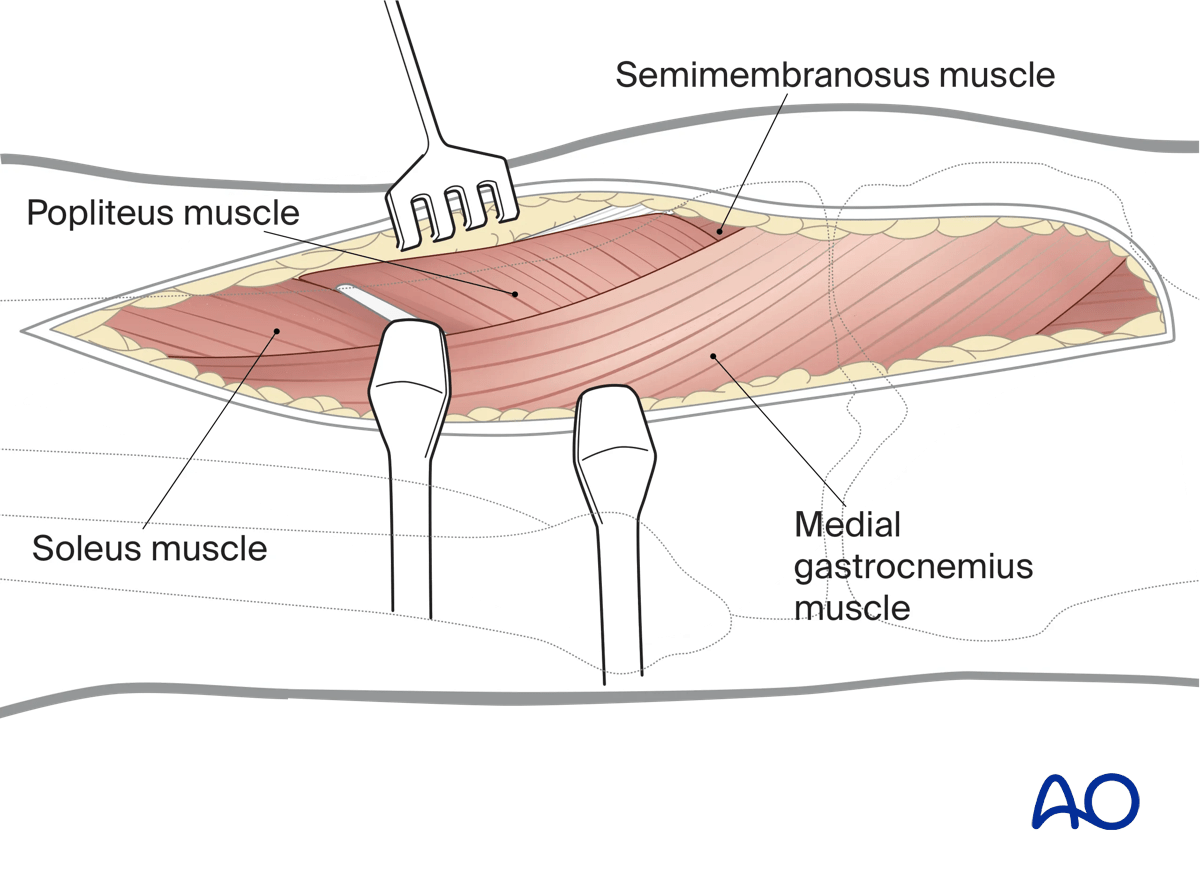
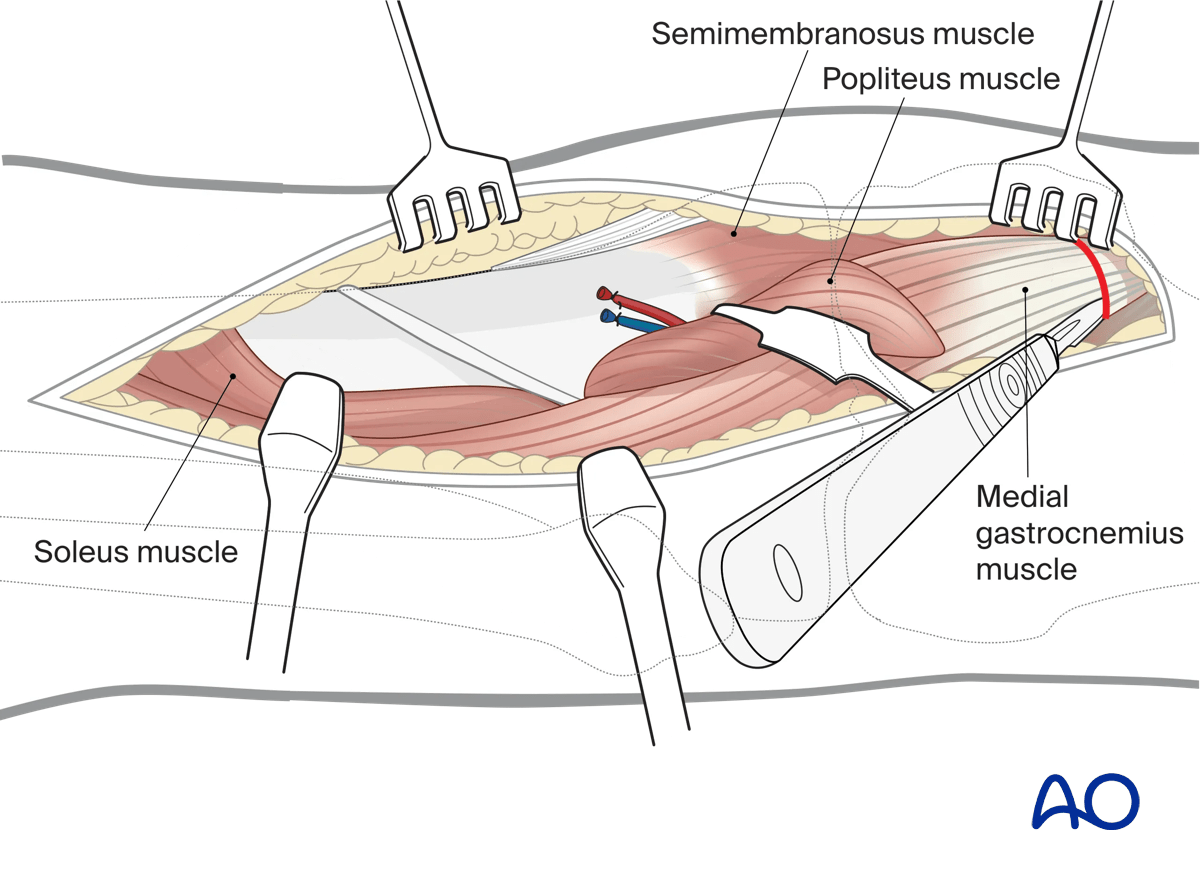
Retract the medial gastrocnemius muscle from medial to lateral and identify the underlying popliteus and soleus musculature. The insertion of the semimembranosus muscle will be seen proximal to the popliteal muscle on the posteromedial aspect of the medial tibial plateau.
Similar to the supine posteromedial approach, the origin of the popliteus muscle and soleus muscle are elevated from the posterior aspect of the tibia from medial to lateral. Hohmann retractors can be carefully placed along the posterolateral tibia to gently retract the soleus and medial gastrocnemius and associated neurovascular structures. It is imperative that the retractors are placed under direct visualization along the osseus surface of the tibia to avoid injury to the vascular structures passing through the interosseus membrane. If increased visualization is required or excessive force is required for retraction, a partial or complete tenotomy of the medial head of the gastrocnemius can be performed.
Intraarticular visualization is limited but can be performed through displacement of fracture fragments. Reduction is typically performed with reliance on extraarticular cortical interdigitations in the epiphysis and metaphysis.
Flexion and extension of the knee can facilitate exposure and reduction strategy.
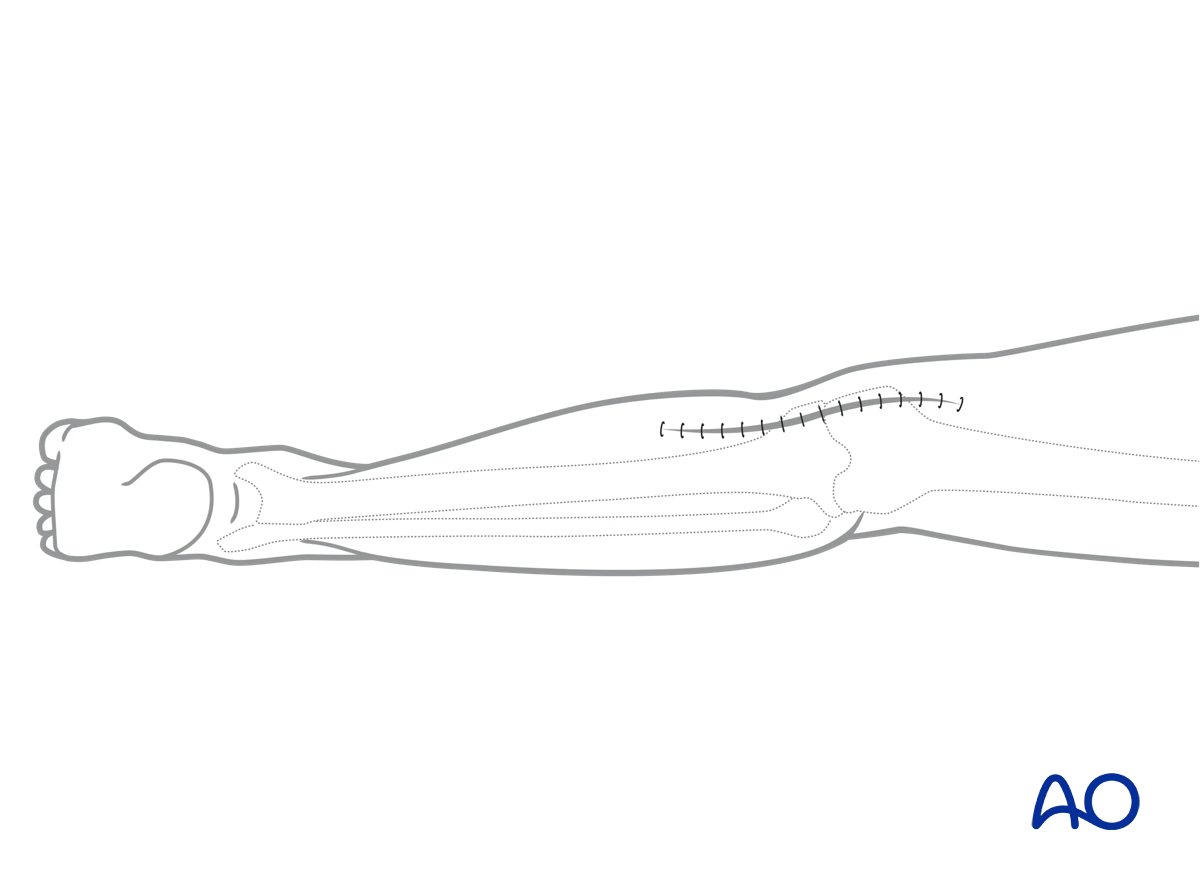
5. Wound closure
Reattach the medial head of the gastrocnemius if required. Place a deep suction drain. Carry out a routine closure of the soft tissues.