ORIF - Conventional plating
1. Principles
General considerations
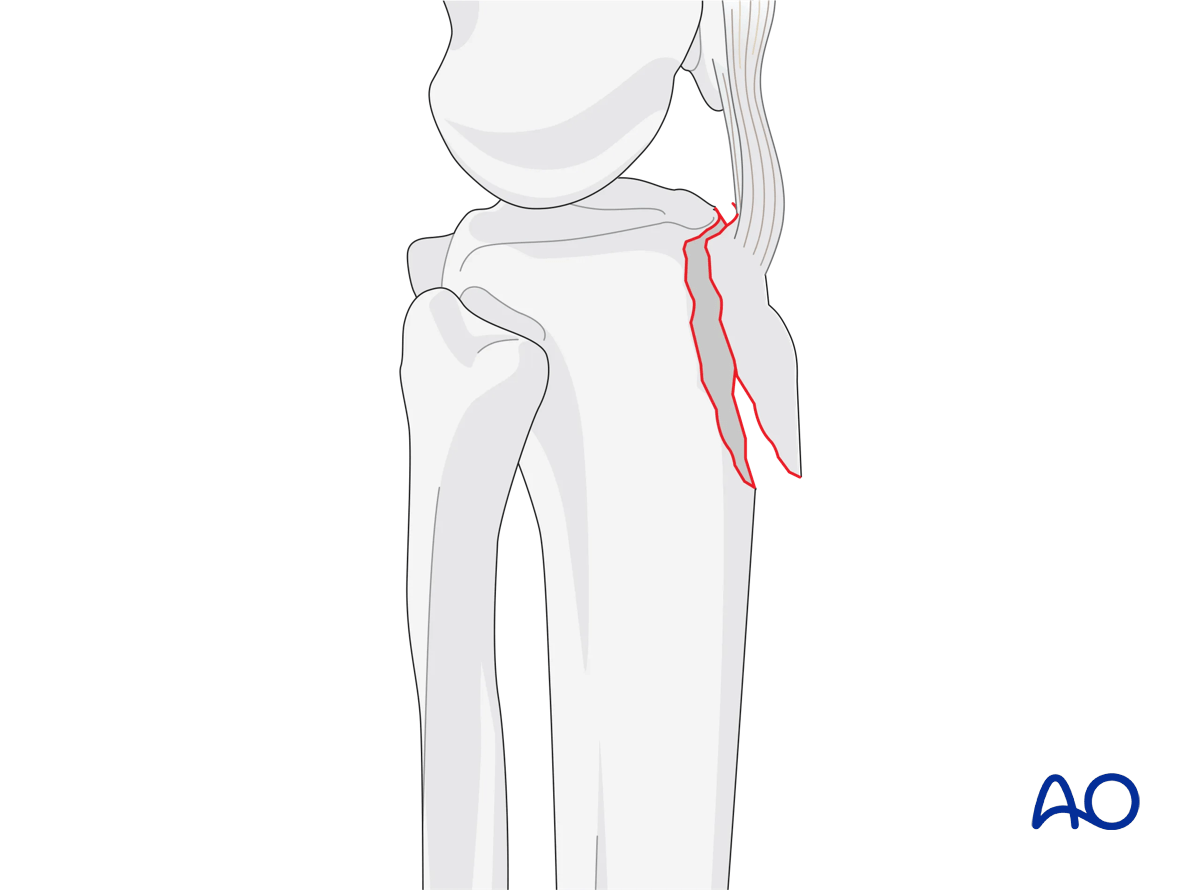
These fractures may occur in isolation, or in conjunction with fractures of the medial and/or lateral tibial plateau. They are often the result of an avulsion force by the extensor mechanism. Large traction forces are exerted on the tibial tubercle, and the surgical construct must therefore be stable to avoid displacement during range of motion and quadriceps contraction.
In situations with severe displacement, the overlying soft tissues and skin may be severely compromised. Unlike other closed proximal tibia fractures, urgent reduction and fixation (definitive or provisional) to prevent skin necrosis may be indicated. Low profile fixation is typically adequate. Suture anchors may be used to augment stability.
Timing of surgery
If local soft tissue is not threatened, surgery should be delayed until patient and operating room personnel are optimized and the limb can be immobilized with a removable knee brace or splint for comfort.
Plate location
Plate location is typically directly anterior, just distal to the insertion of the patella tendon. Plate length should allow for fixation into the anterior portion of the remaining tibia distally.
Potential complications
The following complications should be checked for during surgery:
- Intraarticular hardware
- Prominent fixation
- Compartment syndrome (particularly in skeletally immature patients)
2. Preparation
Patient positioning
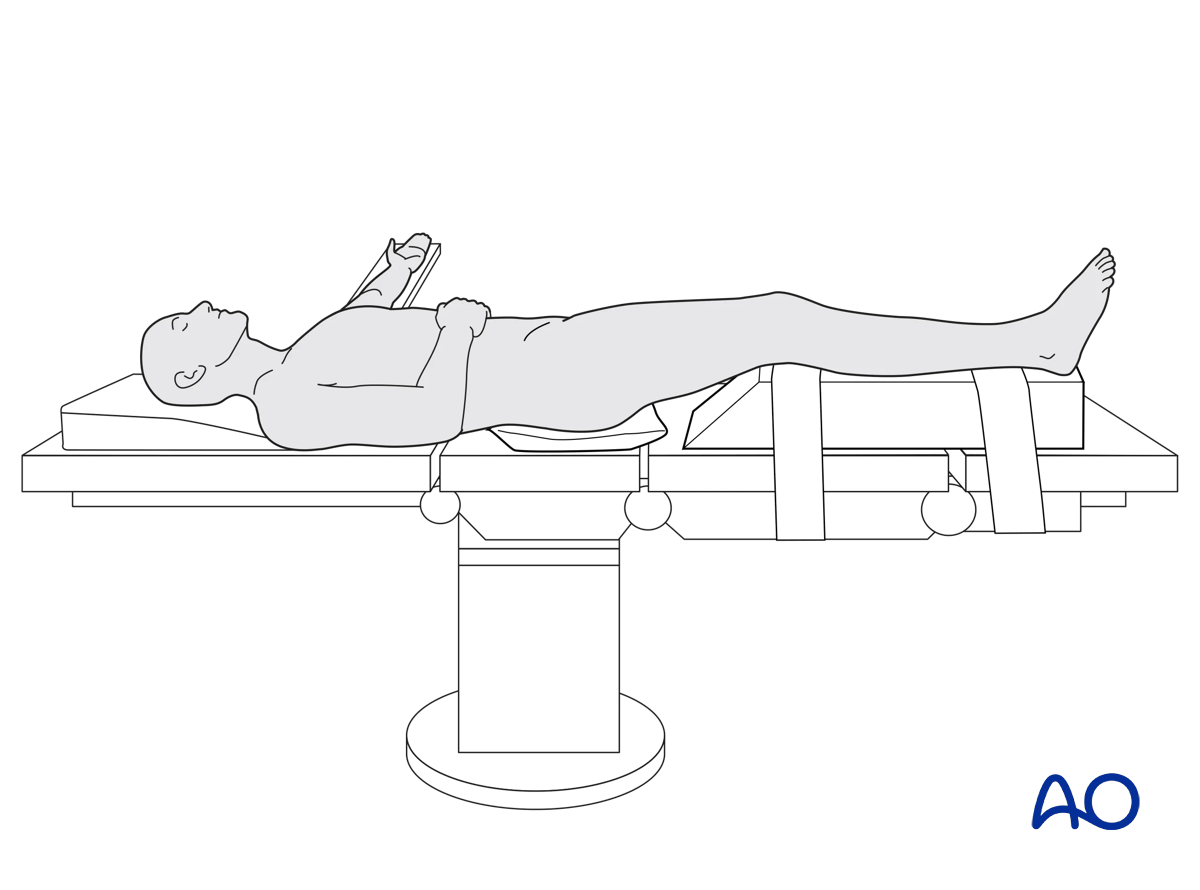
The patient is positioned in the Supine position.
A tourniquet may be helpful in some cases. If used, the tourniquet should be sterile, to allow for intraoperative removal. The majority of tubercle fractures can be fixed without the use of a tourniquet. Whether a tourniquet is used depends on the amount and tolerance of bleeding. Exsanguinate the limb by elevating it.
To allow for intraoperative radiographic control of reduction and fixation, the use of a radiolucent table is mandatory.
3. Approaches
Isolated tibial tubercle fractures can be approached with a straight midline incision. In situations with an associated lateral tibial plateau fracture, the anterolateral approach used for the tibial plateau fracture gives excellent access to the tibial tubercle.
4. Plate application
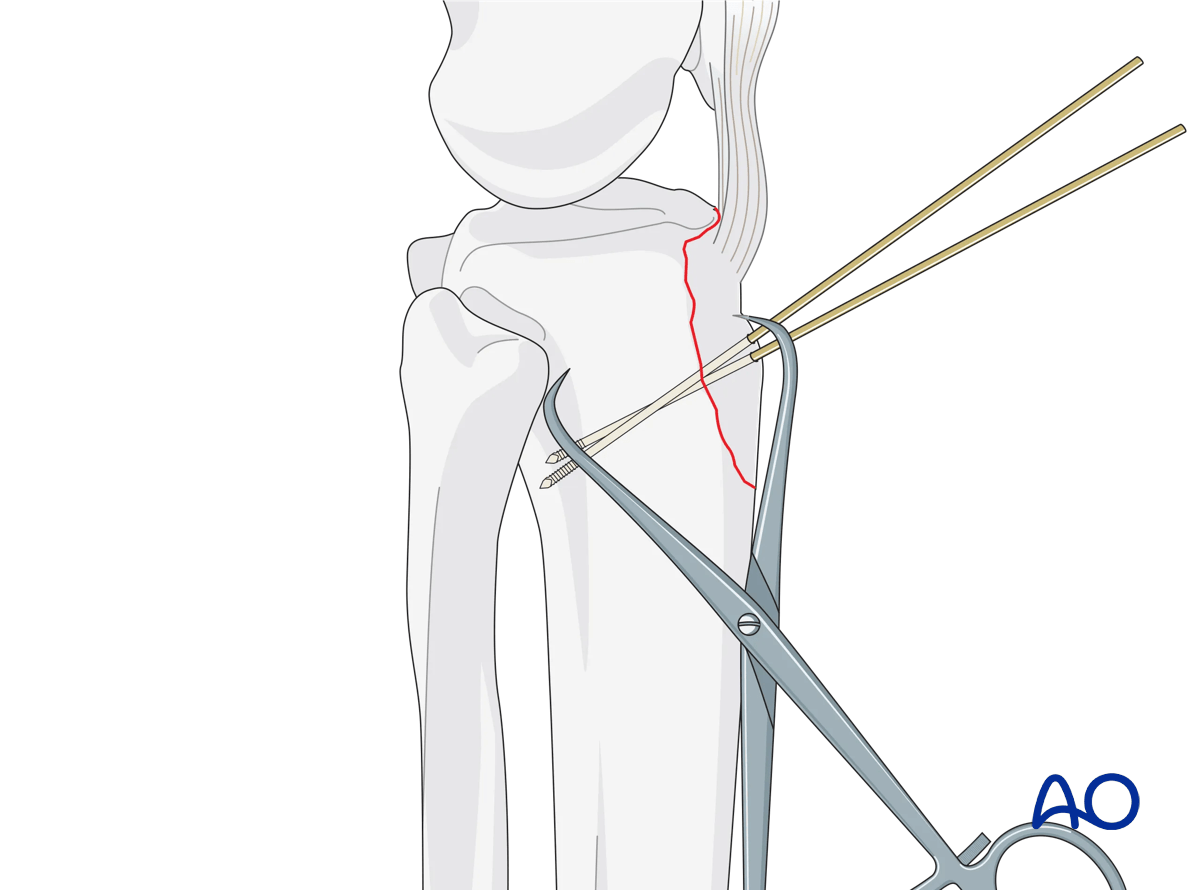
After exposure, the cortical margins are cleansed of their periosteum and the cancellous surface cleansed of its organizing hematoma. The tibial tubercle is reduced with the knee in full extension. Accuracy is assessed using the cortical interdigitations. Once reduced, the K-wires provide provisional stabilization.
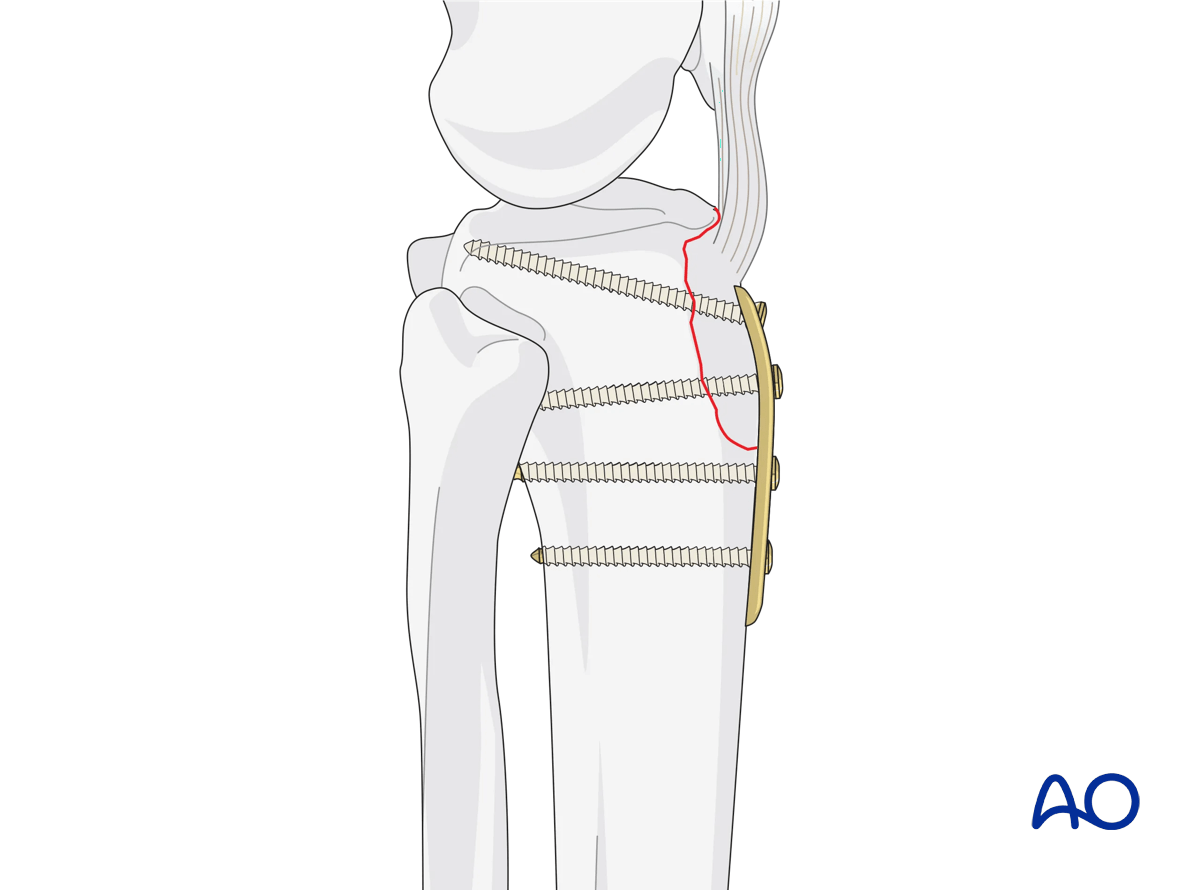
In most instances, low-profile fixation such as 1/3 or 1/4 tubular plates are preferred. The plate is placed to allow fixation beginning at the insertion of the patellar tendon and should cross the fracture line anteriorly distally. Place 3.5 mm lag screws through the plate, across the fracture line. Distally, bicortical fixation secures the tubercle to the tibial shaft.
5. Final osteosynthesis
Once osteosynthesis is completed, make a final check with the image intensifier. If all is well, the knee should then be placed through a full range of motion to ensure fracture stability.
6. Aftercare
Compartment syndrome and nerve injury
Close monitoring of the tibial compartments should be carried out, especially during the first 48 hours after injury and again after surgery to rule out compartment syndrome. More information is provided here:
The neurovascular status of the extremity must be carefully monitored. Impaired blood supply or developing neurological loss must be investigated as an emergency and dealt with expediently.
Consideration for DVT prophylaxis
Oral or subcutaneous administration of DVT prophylaxis for six weeks should be strongly considered.
Functional treatment
Optimal stability should be achieved at the time of surgery, in order to allow early range of motion exercises. Unless there are other injuries or complications, mobilization may be performed on post OP day 1. If available, continuous passive motion (CPM) splints can be very helpful in the early phase of rehabilitation. Static quadriceps exercises with passive range of motion of the knee should be encouraged. Afterwards special emphasis should be given to active knee and ankle movement.
The goal is to achieve as full range of motion as possible within the first 4–6 weeks.
Weight bearing
Weight-of-leg weight bearing is initiated depending on patient comfort. Depending on the severity of the articular displacement, weight bearing can begin as early as 6 weeks postoperatively. In situations where articular displacement was significant weight bearing should be delayed for 10–12 weeks.
Follow up
Wound healing should be assessed within the first two weeks. Subsequently, a 6- and 12-week follow-up with radiographic assessment is usually performed. If a delayed union is recognized, further surgical care may be necessary and should be carried out as soon as possible. Residual knee instability may require delayed reconstruction.
Implant removal
Implant removal is not mandatory and should be discussed with the patient.













