Joint reconstruction of lateral plateau fracture
1. General considerations
Lateral plateau compression fractures need reduction of subchondral fragments. Bone graft and a subchondral screw should be added to support the articular surface.
The lateral avulsion fragment can be stabilized with a position screw or K-wire depending on the fragment size.
The recovery process after such injuries is slow. Advise the patient to expect 6–8 months for full recovery.
2. Patient preparation
Place the patient supine with the arm on a radiolucent hand table.

3. Approach
For this procedure a midaxial approach to the proximal interphalangeal joint is normally used.

4. Reduction
The reduction of the articular fragments can be achieved in different ways depending on the fracture pattern:
- Closed by distraction
- Directly through the fracture
- Directly through a remote entry window (shown here)
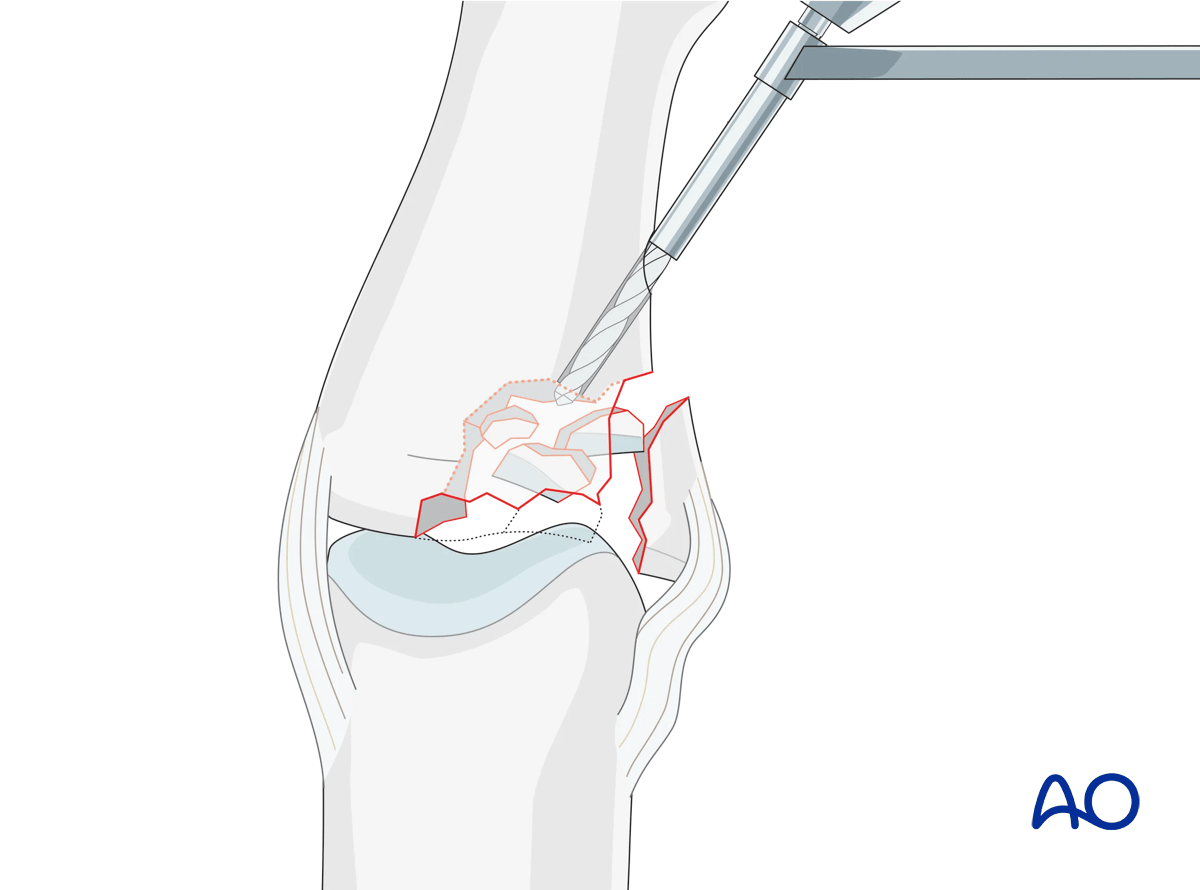
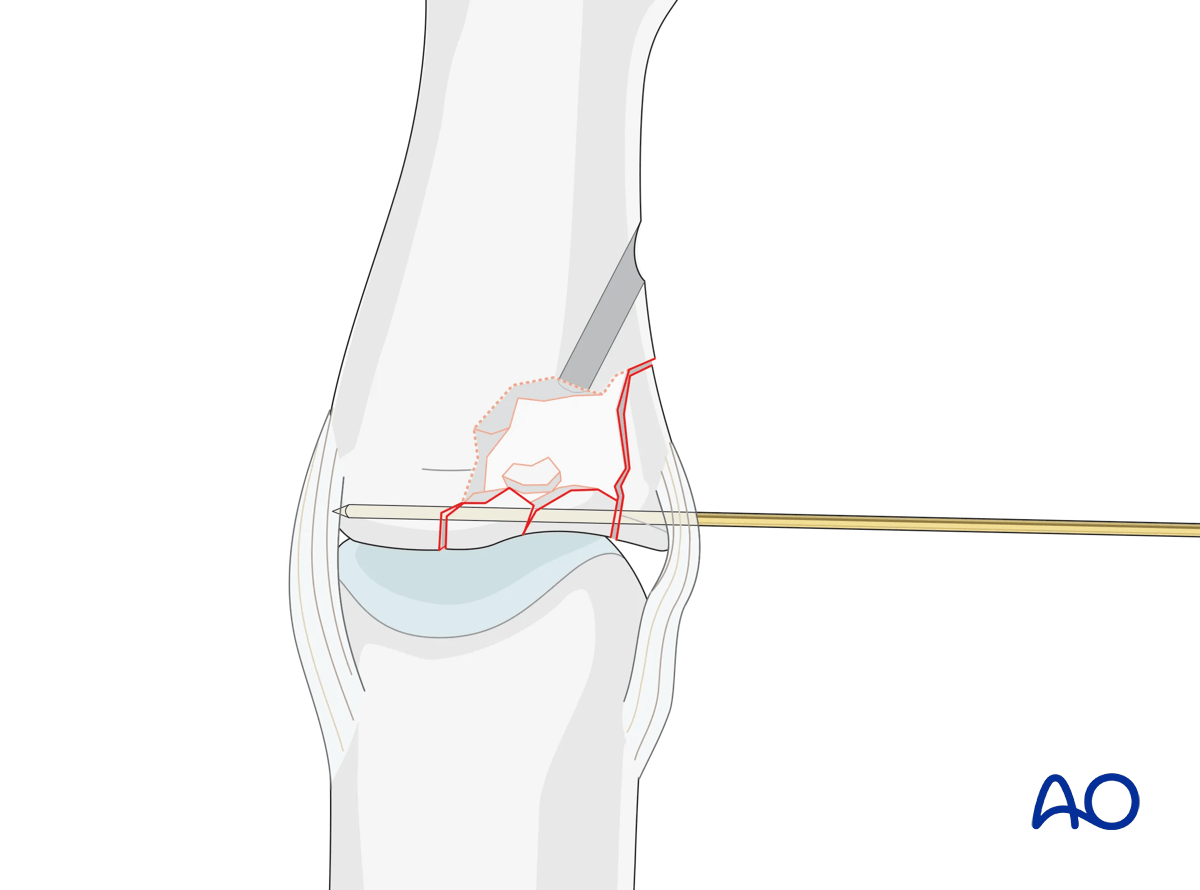
Metaphyseal entry portal
Use a 1.5 mm drill bit to create an entry window just distal to the fracture zone, to permit disimpaction.
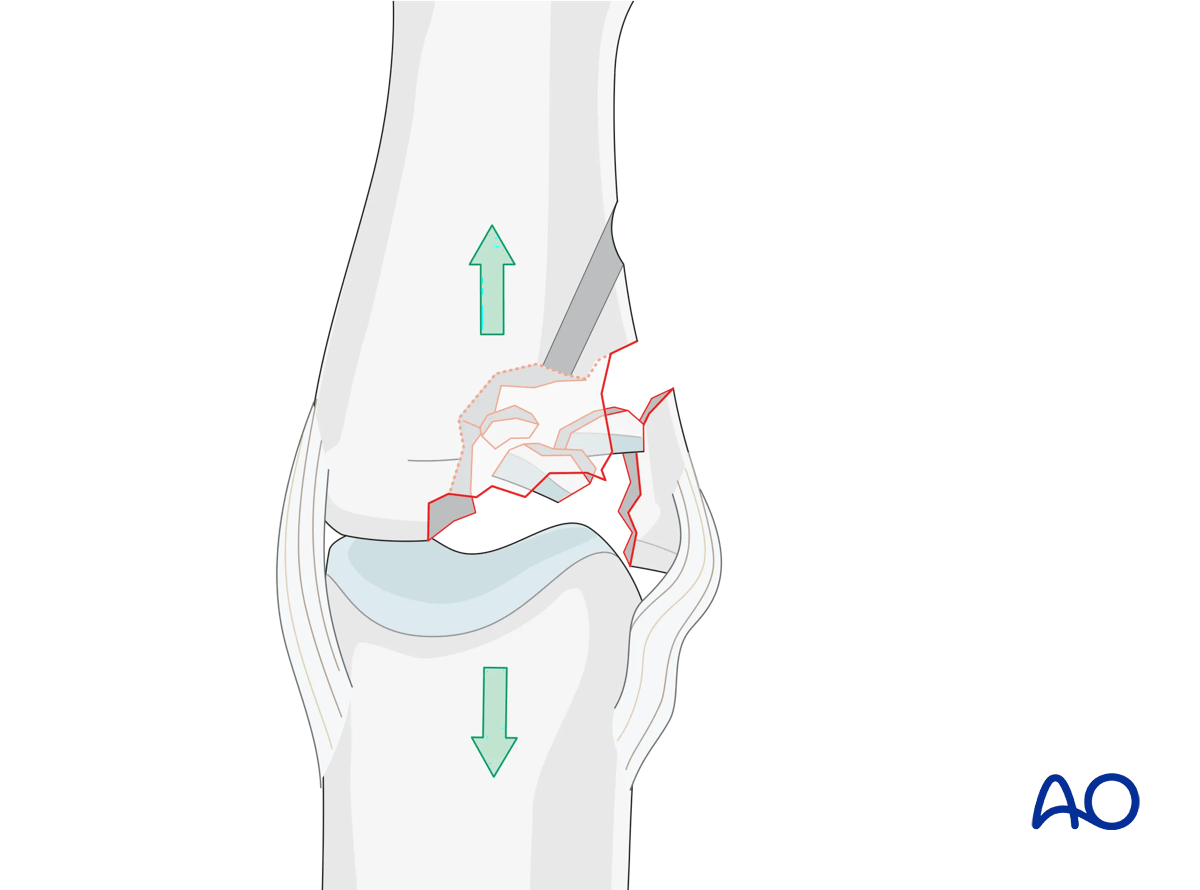
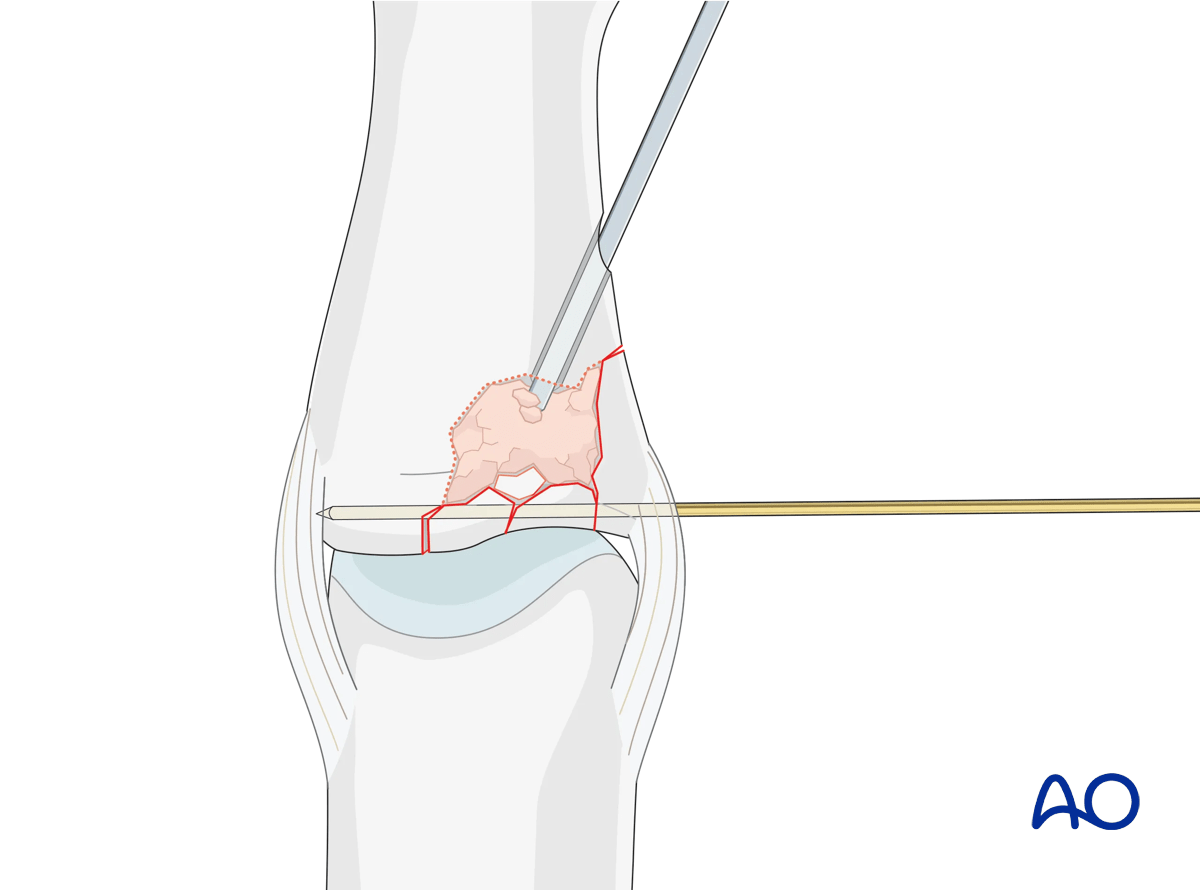
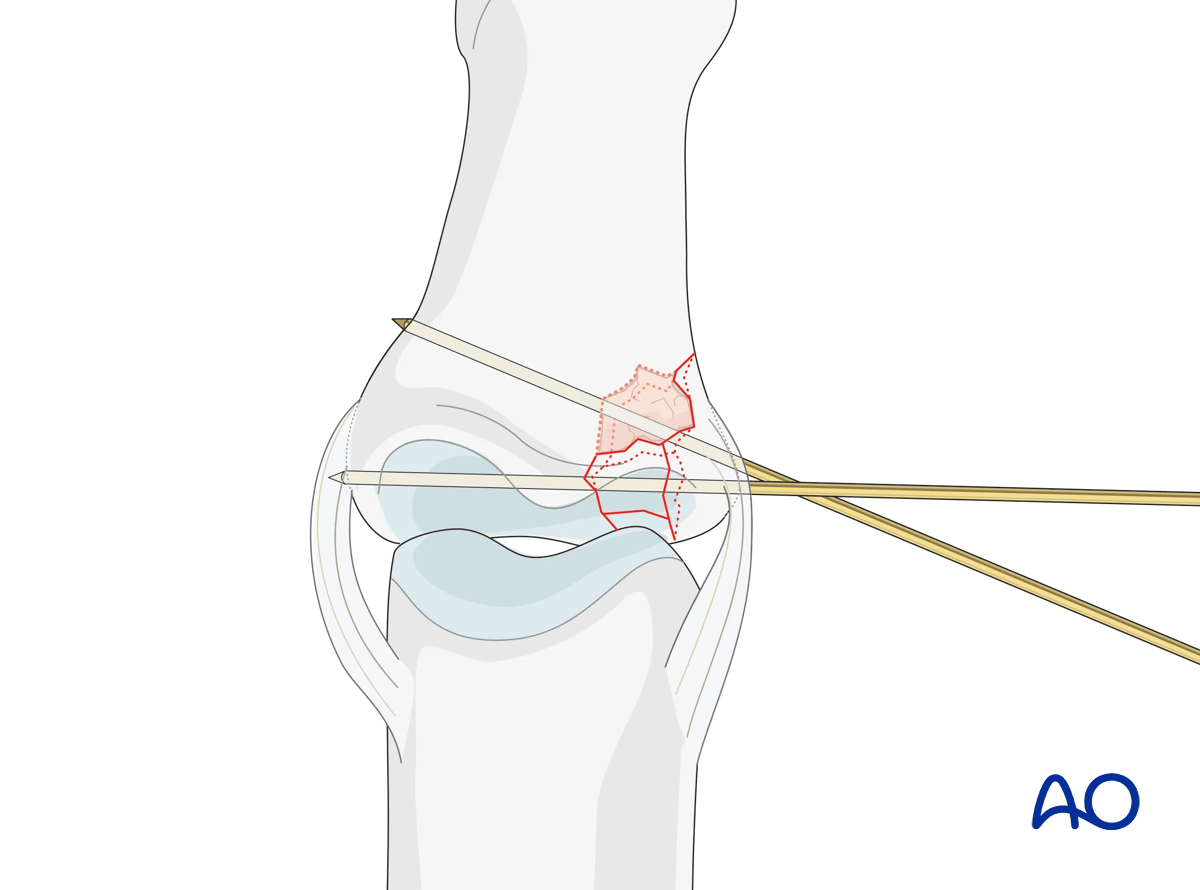
Reduction of the depressed articular fragments
Compression fractures are not reducible by ligamentotaxis, as the centrally impacted fragments are devoid of soft-tissue attachments.
Direct reduction is thus necessary.
The key to fixing compression fractures is restoring the joint surface to as close to normal as possible (anatomically) and supporting the reduction with bone graft.
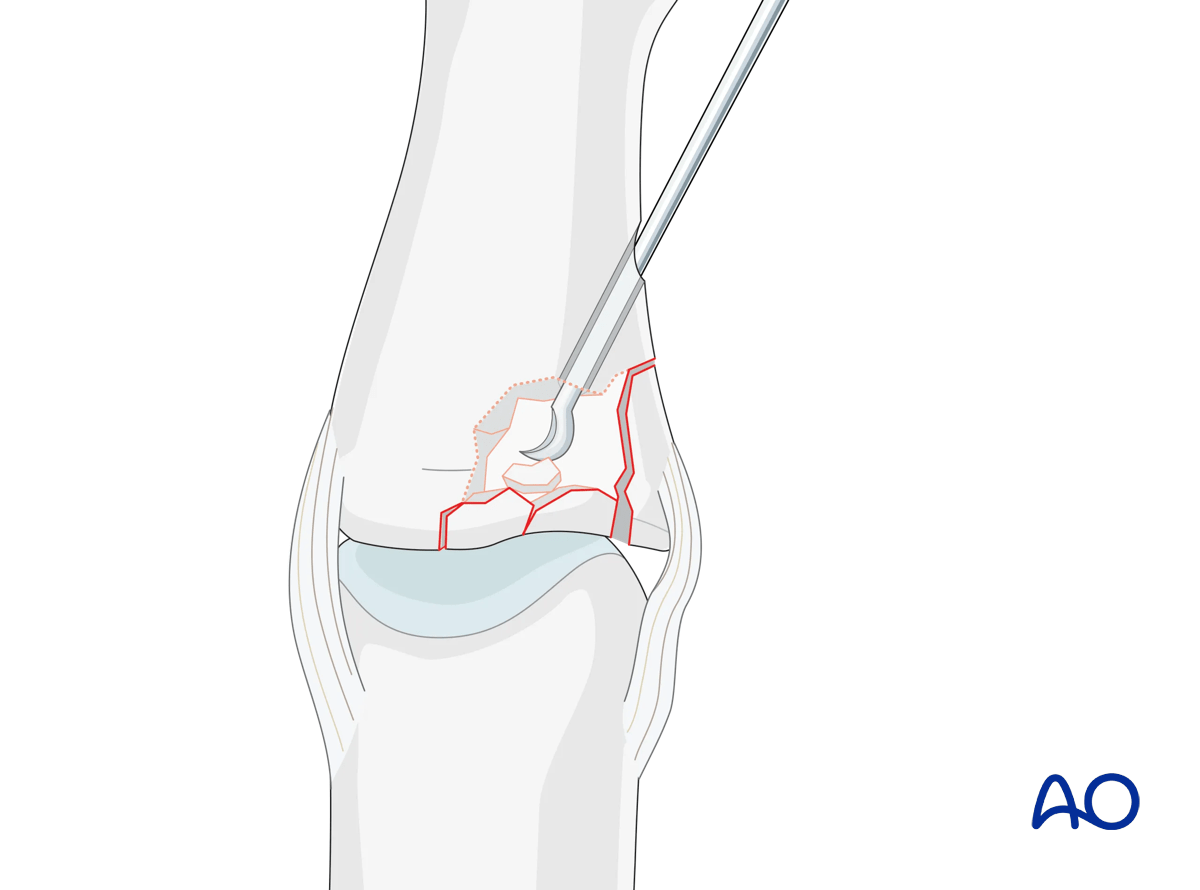
Insert a K-wire, a dental pick, or a tiny curette, into the drill hole. Disimpact the fragments and push them towards the head of the proximal phalanx, which can be used as a template to ensure congruity of the articular surface of the middle phalanx.
If a cartilage step-off remains, degenerative joint disease is likely to follow.
Stabilization of articular fragments
Optionally, insert a K-wire to stabilize the reduction of the articular fragments. This can be left until fracture consolidation.
5. Adding bone graft
Since the subchondral cancellous bone is impacted, a void may remain following reduction of the articular fragments.
This jeopardizes fracture healing:
- Very unstable situation in which the fragments may easily redisplace (collapse)
- Delayed healing process
Therefore, bone grafting is recommended to provide support to the subchondral bone and increase the potential for bone regeneration and healing.
Fill the whole fracture cavity with compacted bone graft, using a blunt dissector.
Confirm reduction with an image intensifier.
6. Fixation
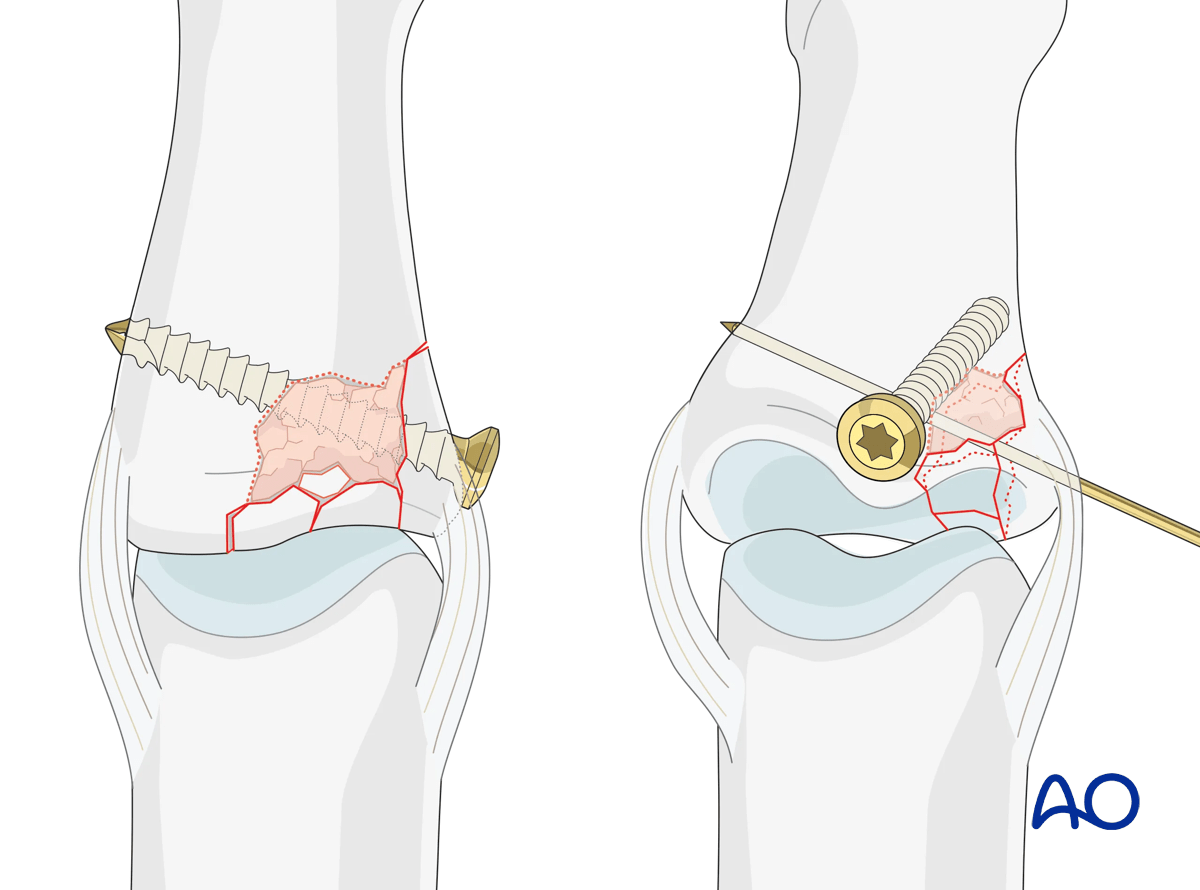
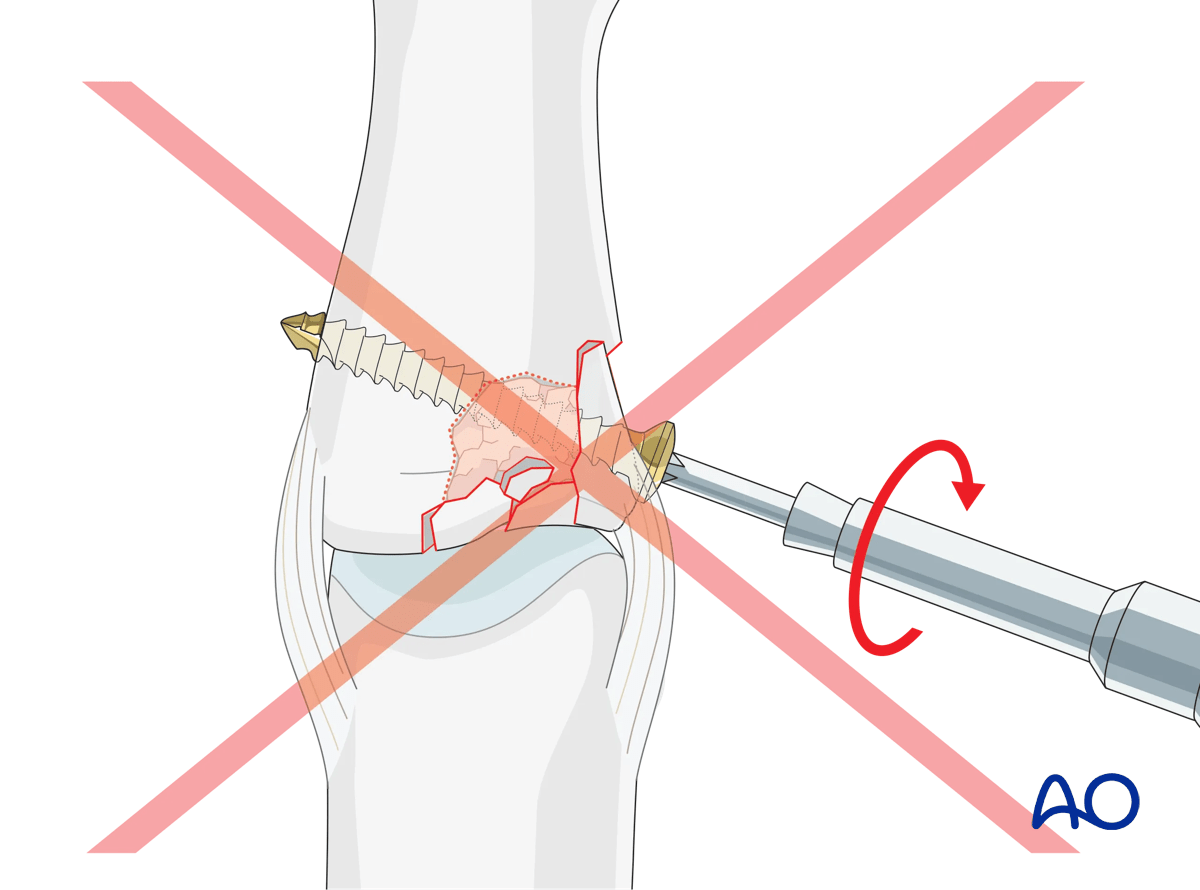
Position screw fixation
If a large lateral fragment is present, maintain its reduction using a position screw (a bicortical cortex screw without lag compression). If the fragment is not large enough, a K-wire may be used, preferably from dorsal to avoid injury to the volar plate.
Maintaining the reduction with slight pressure from a drill guide, drill a threaded hole using the corresponding drill.
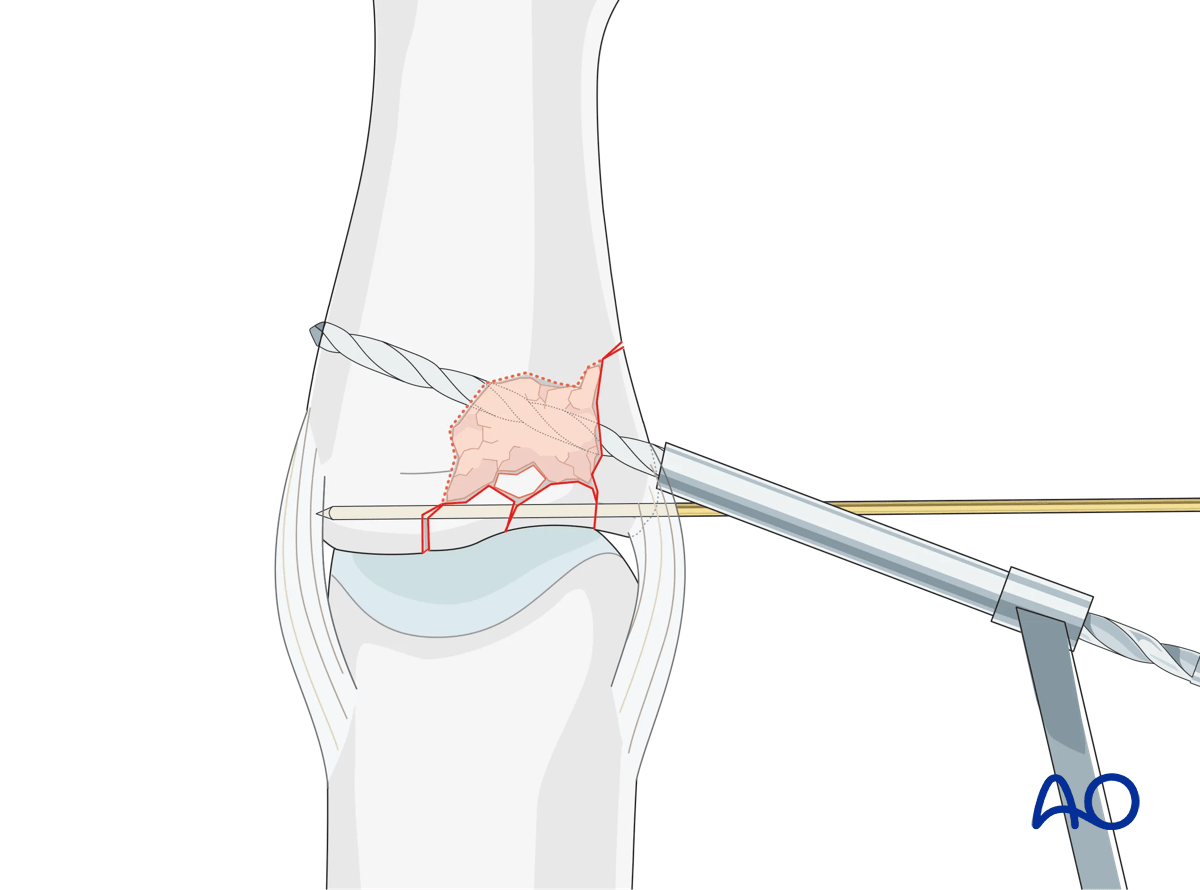
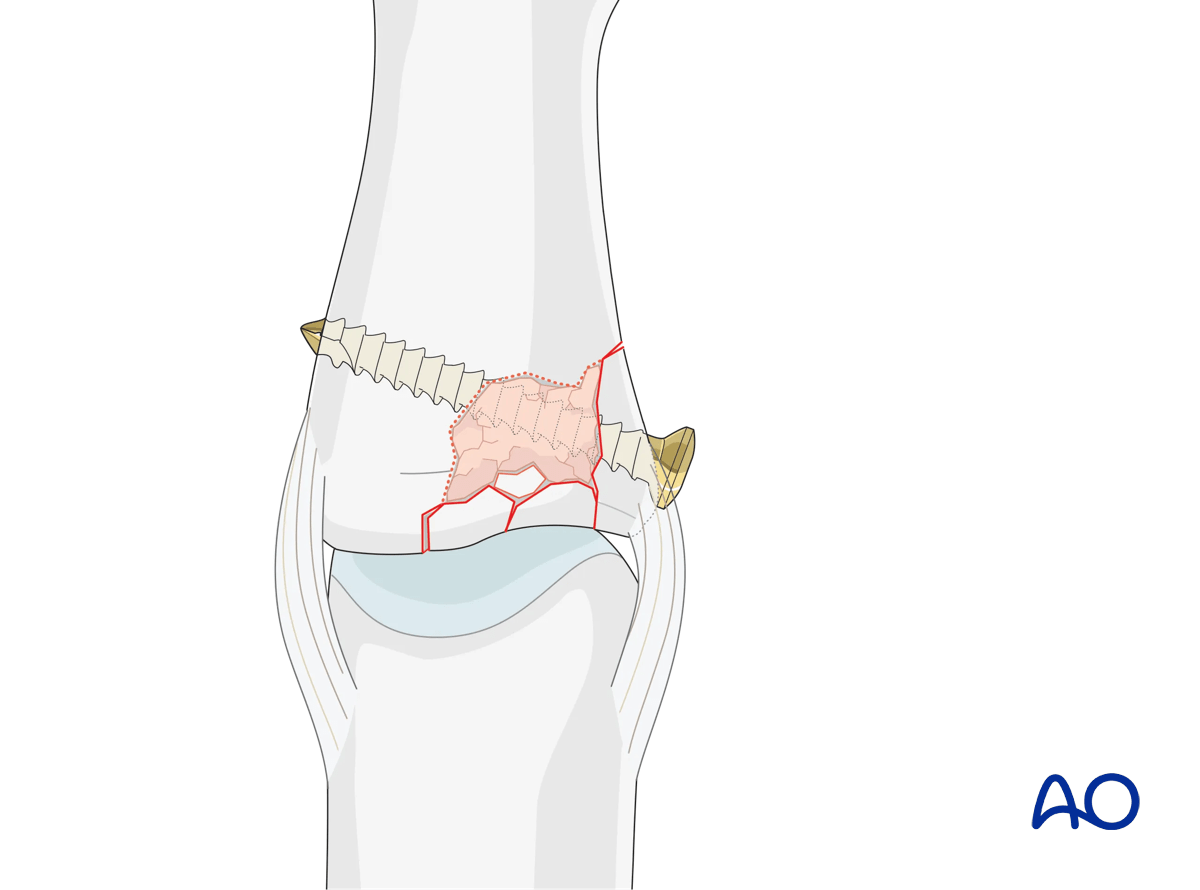
Insert the screw and carefully tighten it just enough to hold the reduction. The screw should just penetrate the opposite cortex.
Check joint congruity using image intensification. Reduction must be anatomical.
K-wire fixation
Stabilize the lateral fragment with one or more K-wires depending on the size of the main fragment.
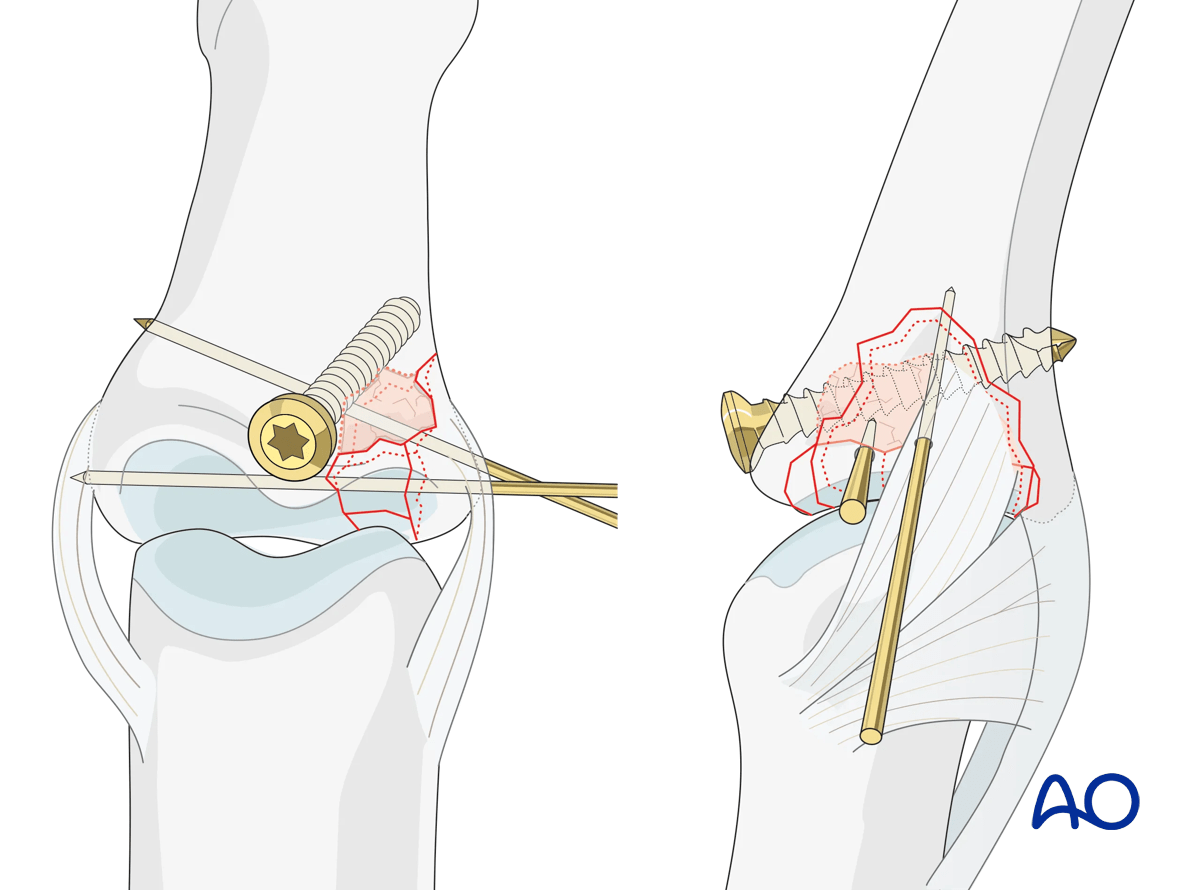
Buttressing
In case of a small cavity, buttressing of the bone graft with one or more K-wires may be considered. In the case of a larger cavity with structured bone graft, a position screw may be used for buttressing.
However, it is preferred to use an antiglide plate.
The screw must be inserted into uninjured palmar cortex and must engage both cortices.
The screw does not need to be inserted parallel to the joint surface. It is more important that it serve to stabilize the reconstruction, and that it has good purchase in both cortices.
Usually, a 1.0 mm or a 1.3 mm screw is used.
Pitfall: tendon irritation

7. Protection of articular reconstruction
Dynamic external fixator
A dynamic external fixator may be added for 4 weeks to keep the PIP joint to length and to allow for early mobilization.

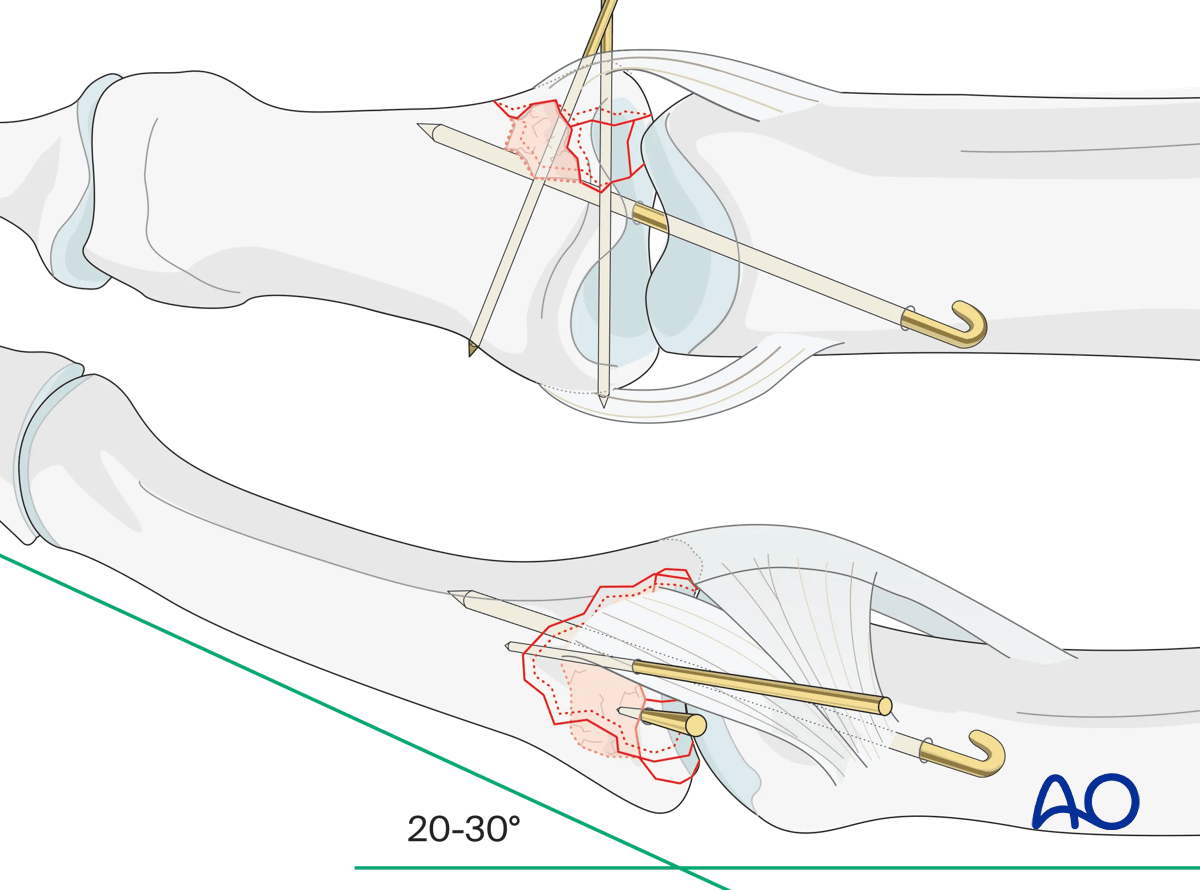
Joint transfixation with K-wire
Following articular reconstruction, if joint instability persists, the PIP joint may be transfixed with a K-wire obliquely, with the joint in 20°–30° of flexion to protect the ligament reattachment. This has a high risk of joint stiffness.
Leave the end of the K-wire outside of the skin for later removal.
The K-wire can be removed after 3–4 weeks.
8. Final assessment
Check joint congruity using image intensification. Reduction must be anatomical.
9. Aftercare
Postoperative phases
The aftercare can be divided into four phases of healing:
- Inflammatory phase (week 1–3)
- Early repair phase (week 4–6)
- Late repair and early tissue remodeling phase (week 7–12)
- Remodeling and reintegration phase (week 13 onwards)
Full details on each phase can be found here.
Postoperatively
If the joint reconstruction has been supported with a dynamic external fixator, additional splinting is not necessary. Early controlled joint mobilization is encouraged.
If joint transfixation has been applied, the hand is immobilized with a dorsal splint for 3–4 weeks. This should permit movement of the unaffected fingers. The arm should be actively elevated to help reduce the swelling.
The hand should be immobilized in an intrinsic plus (Edinburgh) position:
- Neutral wrist position or up to 15° extension
- MCP joint in 90° flexion
- PIP joint in extension

The MCP joint is splinted in flexion to maintain its collateral ligaments at maximal length to avoid contractures.
The PIP joint is splinted in extension to maintain the length of the volar plate.

Follow-up
The patient is reviewed frequently to ensure progression of hand mobilization.
In the middle phalanx, the fracture line can be visible in the x-ray for up to 6 months. Clinical evaluation (level of pain) is the most important indicator of fracture healing and consolidation.
Remove the splint and K-wire after 3–4 weeks and protect the finger with buddy strapping to a neighboring finger to neutralize lateral forces on the finger.

Mobilization
If the fixation is stable enough, the patient is encouraged to take off the splint 2–3 times daily, and to commence with gentle active exercises, provided no transarticular K-wire has been used or has already been removed.
After 4 weeks, the splint (and any K-wire or dynamic external fixator) is removed, and unrestricted active flexion and extension are permitted.

Implant removal
The implants may need to be removed in cases of soft-tissue irritation.
In case of joint stiffness or tendon adhesion restricting finger movement, arthrolysis or tenolysis may become necessary. In these circumstances, the implants can be removed at the same time.













