Open reduction with fixation
1. General consideration
Due to the high incidence of greenstick fractures and the rapid reossification and remodeling, conservative treatment is often the best treatment in a pediatric patient.
Reduction alone may be adequate in some pediatric zygomaticomaxillary complex (ZMC) fractures due to the higher incidence of greenstick fractures. Moreover, multibuttress reconstruction is also less frequently indicated.
2. Approach
A vestibular incision is most commonly used to approach these fractures. A combination of lower eyelid incision and upper blepharoplasty incision may be added depending on the severity and the displacement of the fracture.
3. Reduction
The height, width, and projection of the midface should be restored.
Reduction is performed as in the adult population.
4. Fixation
Fixation of the zygomaticomaxillary buttress will usually offer adequate rigidity in simple pediatric ZMC fractures. More complex ZMC fractures can be addressed as it is done in the adult population.
Care must be given to avoid tooth buds with screws when plating. Moreover, excessive undermining and periosteal stripping can alter the growth potential of the midface in young children.
Choice of internal fixation
ORIF of ZMC fractures is conducted in a stepwise fashion. If 1-point fixation is not adequate to reestablish normal anatomy and stability, then 2-point fixation is used. If 2-point fixation is still not sufficient, a 3-point fixation is done.
Orbital evaluation and reconstruction are done on an as-needed basis, depending on functional and anatomical deficits.
Due to the higher incidence of muscle entrapment in pediatric orbital fractures, orbital reconstruction may sometimes be indicated regardless of ZMC fracture severity.
Unstable ZMC fractures in children are treated as in the adult population.
5. Aftercare
Patient vision is evaluated on awakening from anesthesia and then at regular intervals until hospital discharge.
A swinging flashlight test may serve in the unconscious or noncooperative patient; alternatively, an electrophysiological examination has to be performed but is dependent on the appropriate equipment (VEP).
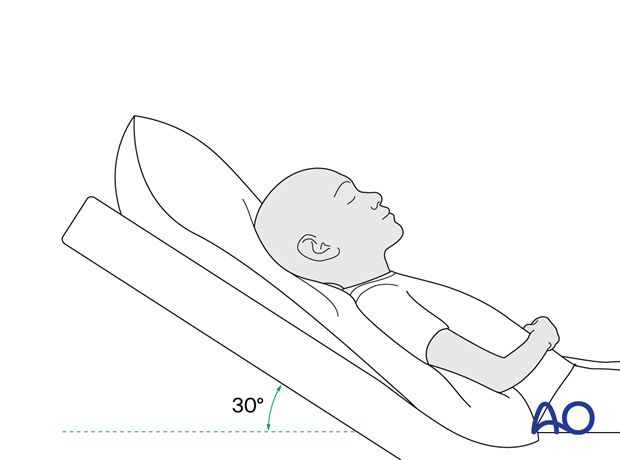
Postoperative positioning
Keeping the patient’s head in an upright position both preoperatively and postoperatively may significantly improve periorbital edema and pain.
Nose blowing
Nose blowing should be avoided for at least ten days following orbital fracture repair to prevent orbital emphysema.
Medication
The use of the following perioperative medication is controversial. There is little evidence to make solid recommendations for postoperative care.
- No aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs) prescribed for seven days.
- Provide analgesia as necessary.
- Antibiotics (many surgeons use perioperative antibiotics. There is no clear advantage of any antibiotic, and the recommended duration of treatment is debatable.)
- A nasal decongestant may be helpful for symptomatic improvement in some patients.
- Steroids, in cases of severe orbital trauma, may help with postoperative edema. Some surgeons have noted increased complications with perioperative steroids.
- Regular perioral and oral wound care must include disinfectant mouth rinse, lip care, etc.
Ophthalmological examination
Postoperative examination by an ophthalmologist may be requested. The following signs and symptoms are usually evaluated:
- Vision
- Extraocular motion (motility)
- Diplopia
- Globe position
- Visual field examination
- Lid position
- If the patient complains of epiphora (tear overflow), lacrimal duct function must be checked.
Postoperative imaging
Postoperative imaging has to be performed within the first days after surgery. 3D imaging (CT, cone beam) is recommended to assess complex fracture reductions. An exception may be made for centers capable of intraoperative imaging.
Wound care
Ice packs are effective in the short term to minimize edema.
Remove the sutures from the skin after approximately five days if non-resorbable sutures have been used.
Avoid sun exposure and tanning to skin incisions for several months.
Clinical follow-up
Clinical follow-up depends on the complexity of the surgery and whether the patient has any postoperative problems.
With patients having fracture patterns including periorbital trauma, issues to consider are the following:
- Globe position
- Double vision
- Other vision problems
Other issues to consider are:
- Facial deformity (incl. asymmetry)
- Sensory nerve compromise
- Problems of scar formation
Eye movement exercises
Following orbital fractures, eye movement exercises should be considered.
Implant removal
Generally, orbital implant removal is not necessary except in the event of infection or exposure.
Oral hygiene
A soft toothbrush (dipped in warm water to make it softer) should be used to clean the surfaces of the teeth Chlorhexidine oral rinses or nonalcoholic mouth wash should be prescribed and used at least three times a day and after meals to help sanitize the mouth.
Special considerations for orbital fractures
Travel in commercial airlines is permitted following orbital fractures. Commercial airlines pressurize their cabins. Mild pain on descent may be noticed.
No scuba diving should be permitted for at least six weeks.
Children who participate in sports should consider wearing eye protection for the first three months following the fracture.
Special considerations for pediatric ZMC orbital fractures
Children who participate in sports should consider wearing eye protection for the first three months following the fracture and contact sport should be avoided for the first six weeks.
6. Case example
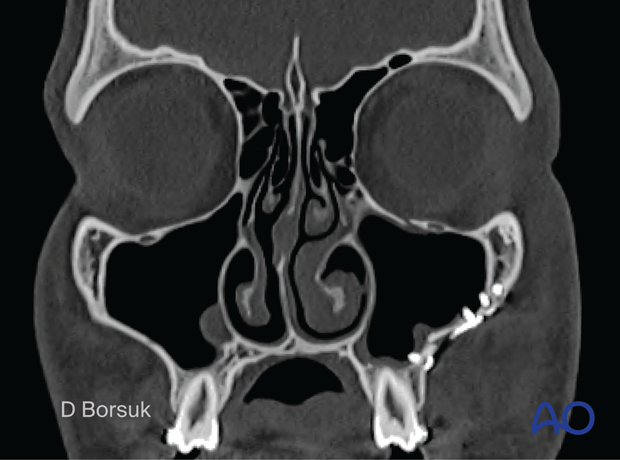
A 15-year-old male patient with left depressed ZMC orbit fracture.
Coronal view of left displaced ZMC orbital fracture. Note the greenstick fracture of the zygomaticofrontal suture and the minimally displaced orbital floor fracture.
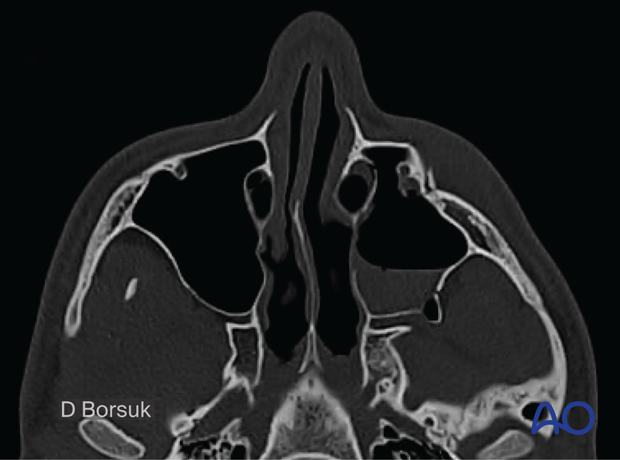
Axial view of the same fracture displaying loss of facial width and projection.
Note the greenstick fracture of the zygomatic arch.
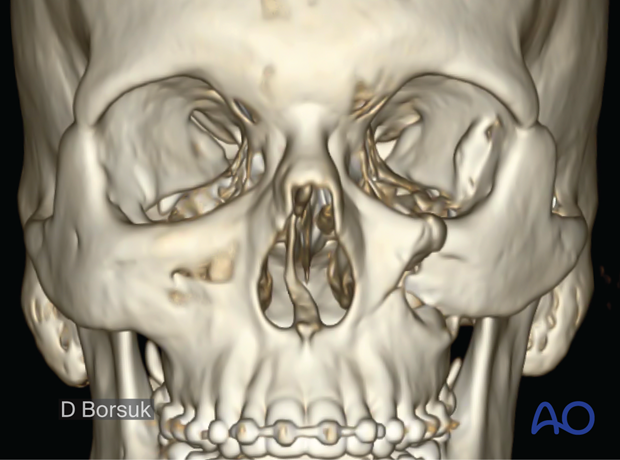
Postoperative 3D scan following 1-point fixation of the zygomaticomaxillary buttress. Due to the greenstick fractures, relative bony stability, and rapid healing in children, the 1-point fixation was adequate in restoring and maintaining the height, width, and projection of the midface.

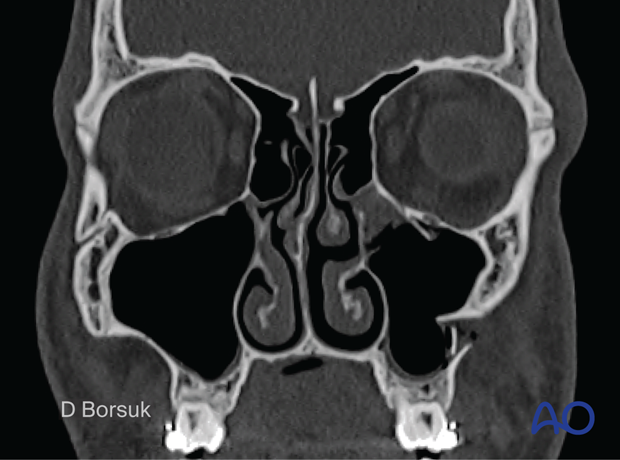
Postoperative coronal view displaying 1-point fixation of the zygomaticomaxillary buttress with the restoration of the orbital floor and midface width.