Open reduction internal fixation
1. Special considerations for pediatric patients
Due to the growth potential, the presence of tooth buds, and the rapid healing, pediatric surgical Le Fort fractures have special considerations:
- Fractures should be approached through limited exposure to avoid devascularizing the bone and affecting the growth potential.
- Small monocortical screws should be used to avoid injury to the developing tooth buds.
- Non-bioresorbable hardware should be removed once the fracture has healed.
- One plate on the lateral zygomaticomaxillary buttress may be adequate for providing stability in children.
2. Approach
Maxillary vestibular incisions are most commonly used to address Le Fort fractures.
A coronal incision is frequently used to address the nasal-frontal buttress and a lid incision can be used to access the orbital rim.
Care is taken not to overexpose the bone to avoid harming growth potential.
3. Reduction
All midface fracture reduction's primary goal is to restore function, ie, dental occlusion, facial height, width, and projection.
The open reduction technique is performed as in the adult population.
4. Fixation
Careful fixation with small monocortical screws should be done to avoid tooth buds. Intraoperative navigation or CT scan can be considered to help avoid the tooth buds.
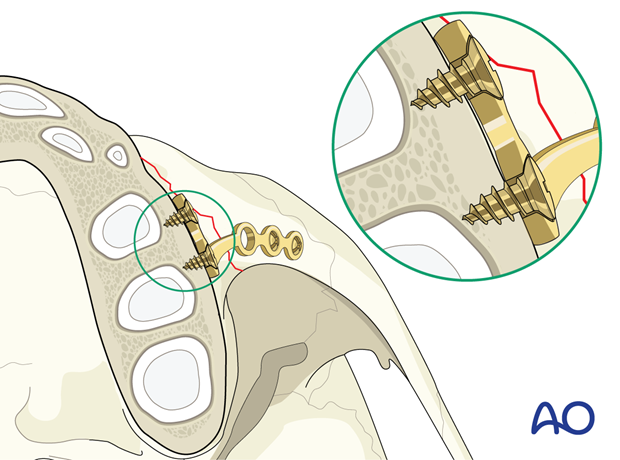
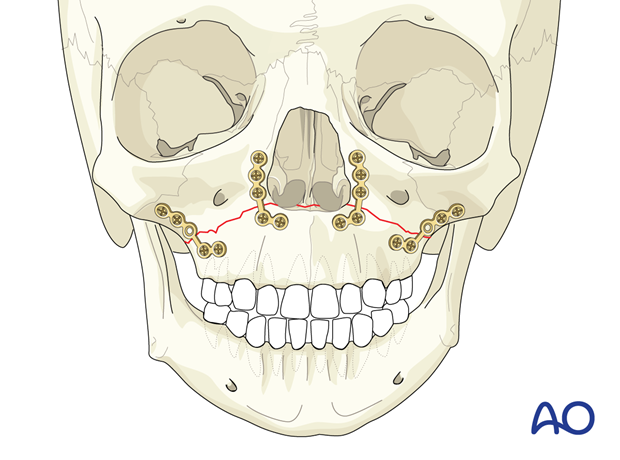
The maxilla should be plated at the lateral, medial vertical buttresses, where the bone is thickest.
Since the soft bony callus will form and stabilize the fracture between 1 and 2 weeks, multiple plates are rarely required.
5. Aftercare
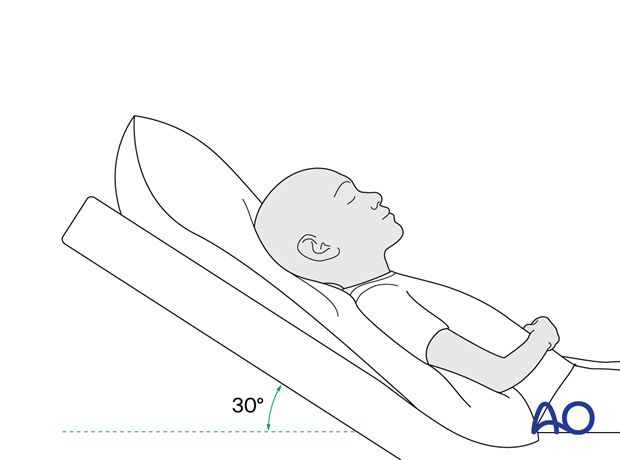
Postoperative positioning
Keeping the patient's head in an upright position both preoperatively and postoperatively may significantly improve periorbital edema and pain.
Medication
The use of the following perioperative medication is controversial. There is little evidence to make solid recommendations for postoperative care.
- No aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs) prescribed for 7 days.
- Provide analgesia as necessary.
- Antibiotics (many surgeons use perioperative antibiotics. There is no clear advantage of any antibiotic, and the recommended duration of treatment is debatable.) More information can be found in the article: Mundinger GS, Borsuk DE, Okhah Z, et al. Antibiotics and facial fractures: evidence-based recommendations compared with experience-based practice. Craniomaxillofac Trauma Reconstr. 2015 Mar;8(1):64-78.)
- A nasal decongestant may be helpful for symptomatic improvement in some patients.
- Regular perioral and oral wound care must include non-alcoholic disinfectant mouth rinse, lip care, etc.
Postoperative imaging
Postoperative imaging should be performed within the first days after surgery to assess reductions and possible malpositioning. 3D imaging (CT, cone beam) is recommended to assess complex fracture reductions. An exception may be made for centers capable of intraoperative imaging.
Especially in fractures involving the alveolar area, orthopantomograms (OPG) are helpful.
Wound care
Ice packs are effective in the short term to minimize edema. Avoid sun exposure and tanning to skin incisions for several months.
Diet
Diet depends on the fracture pattern.
A soft diet can be taken as tolerated until adequate healing of the maxillary vestibular incision.
Nasogastric feeding may be considered in children who refuse to be fed through their mouth.
Clinical follow-up
Children should be followed up within a week after the surgery and once the fracture has healed to ensure normal weight gain and proper oral hygiene.
Children should be assessed throughout adolescence to ensure no facial asymmetries and growth disturbances occur. Dental development and occlusion should be evaluated, and appropriate consultation with pedodontics and orthodontics should be considered when applicable.
Implant removal
Implant removal should be considered in children under the age of eight to ensure that tooth eruption and facial growth are not disturbed.
Oral hygiene
A soft infant toothbrush should be used to clean the teeth surfaces. Nonalcoholic oral mouth wash should be prescribed and used at least three times a day and after meals to help sanitize the mouth.













