Nonoperative treatment
1. No immobilization and early motion
Indications
Nonoperative treatment of these fracture patterns is unusual, but occasionally appropriate. The following are patient characteristics that are relative indications for nonoperative treatment:
- Low-functional status
- Advanced medical comorbidities
- Significant preexisting arthrosis of the knee
- Advanced osteoporosis
The following are relative fracture pattern indications for nonoperative treatment:
- Articular displacement of less than 2–5 mm
- Widening of less than 5 mm
- Less than 5° of frontal and/or sagittal plane malalignment
- Metaphyseal displacement of less than 5–10 mm
However, even in situations where these criteria are satisfied, these fracture patterns are inherently unstable, and close radiographic follow-up is required. Additionally, operative treatment may still be chosen in the setting of neurovascular injury, compartment syndrome, a multiply injured patient, associated injuries of the limb, etc.
2. Posterior plaster splint
Indication
Seven to ten days of long-leg posterior plaster splinting is indicated, with the knee in 0–20° of flexion as comfort allows. Patients can then be transitioned to a knee immobilizer or hinged knee brace and begin range of motion exercises.
These fractures are more severe, and so immobilization for up to three weeks may be required, prior to beginning significant range of motion exercises.
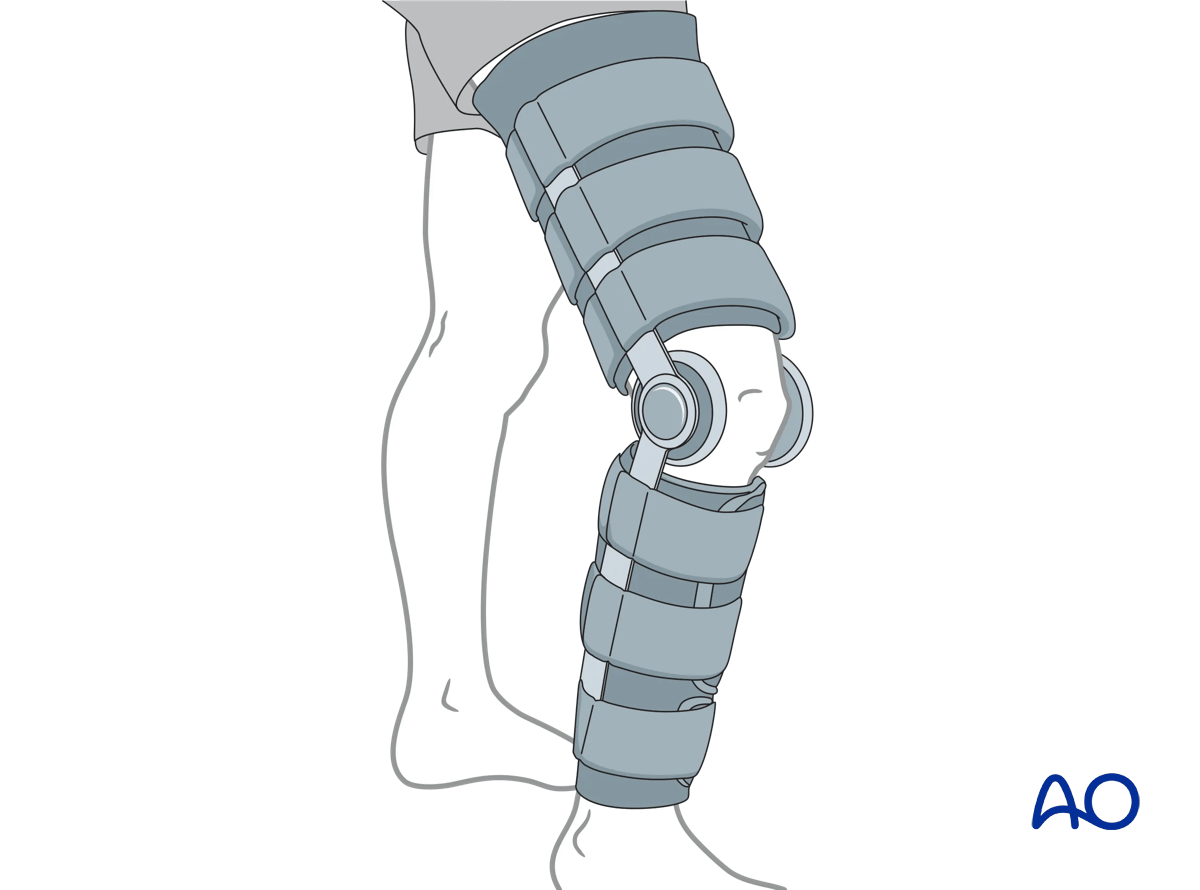
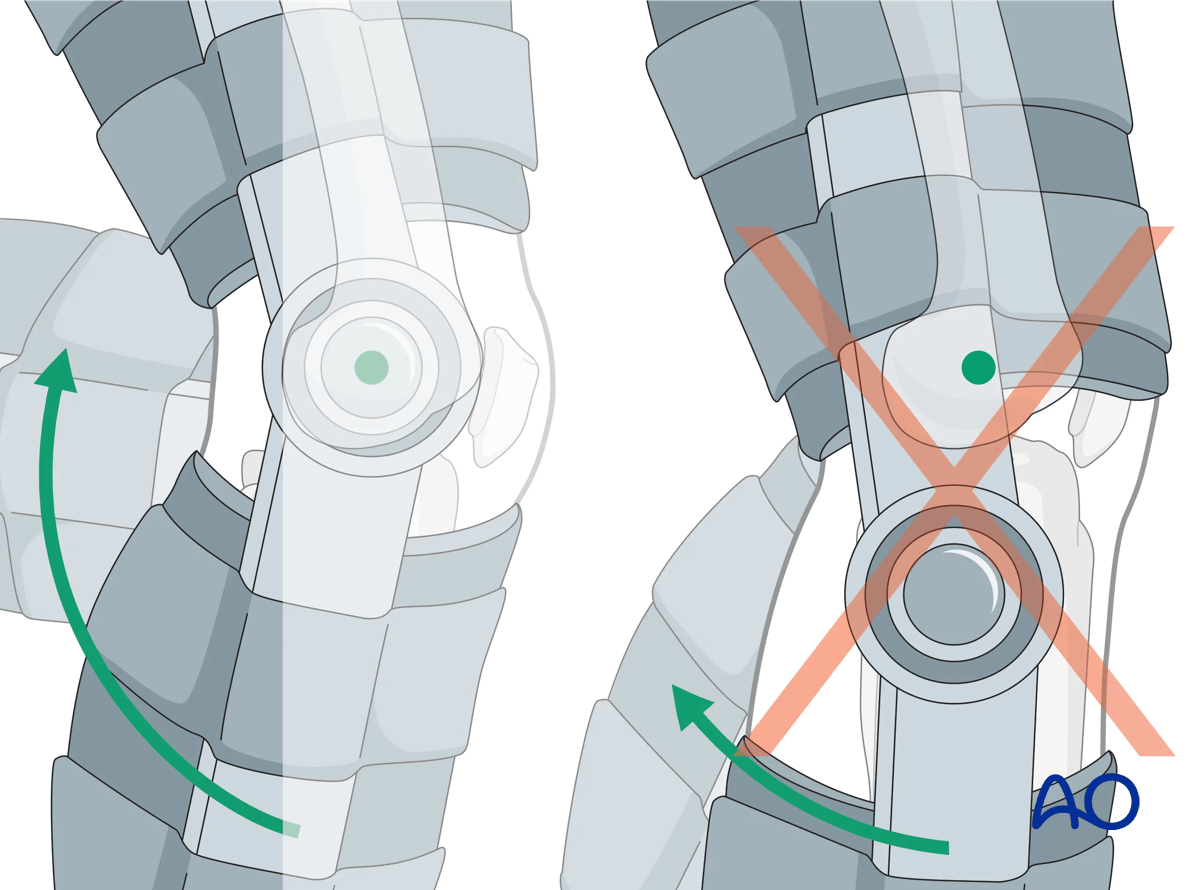
3. Knee immobilizer and hinged fracture brace
Indication
These devices provide relative immobilization of the knee joint, allowing pain relief. Regardless of the device used, patients must be instructed to begin knee range of motion exercises as pain subsides, typically beginning within one to two weeks. During this time, ankle range of motion is to be encouraged, as are quadriceps setting exercises, and straight leg raising. These devices can be used for all fractures as a means of temporary splinting.
4. Aftercare
Patients should take off the immobilizer, or knee brace, for hygiene, quiet time, and range of motion.
DVT prophylaxis should be considered and addressed in both nonoperatively and operatively managed patients.
Aftercare and rehabilitation following nonoperative treatment should be individualized according to the patient, fracture, and local protocol specifics.
Pain and neurovascular status should continue to be monitored, particularly in the immediate post-injury time period. Active motion of the joint should begin within 7–14 days. Full weight bearing is often restricted for 6–10 weeks.
Early weekly radiographic follow-up should be considered to ensure there is no change in alignment.













