Closed treatment
1. General consideration
Due to the high incidence of greenstick fractures and the rapid reossification and remodeling, nonoperative treatment is often the best treatment in non-displaced pediatric nasal fractures.
In displaced fractures, however, an early reduction should be considered due to rapid pediatric bone healing. Nasal swelling does not preclude early reduction. Once a displaced nasal fracture is diagnosed, it should be reduced.
A closed reduction is difficult to perform in children under local anesthesia. Therefore, general anesthesia with proper airway control is often the safest and the best way to address displaced pediatric nasal fractures.
In cases of a delayed diagnosis of a displaced pediatric nasal fracture, open reduction should be considered, regardless of fracture date. The potential disturbance in nasal growth should not dissuade an attempt at anatomic reduction.
2. Reduction
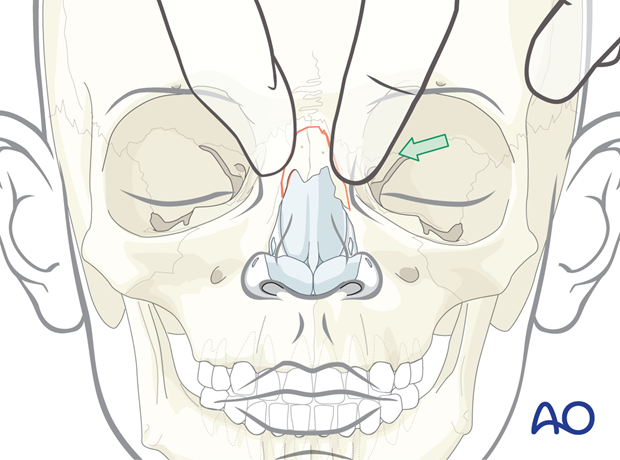
Most pediatric nasal fractures are greenstick in nature. The nasal bone pyramid is commonly shifted to one side without nasal bone collapse.
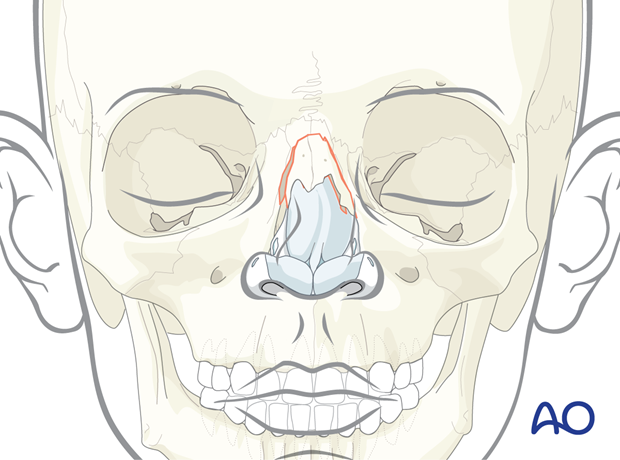
These fractures can be reduced with external manipulation only.
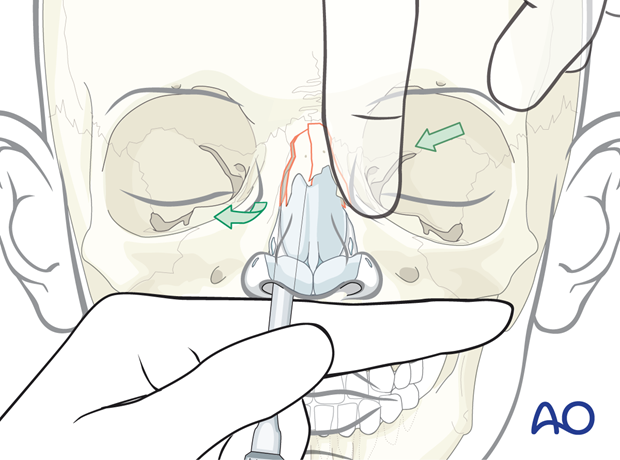
If, however, there is nasal bone collapse, a combined intranasal and external approach may be required.
The surgical reduction is performed as for adults.
3. Splinting
Nasal bones
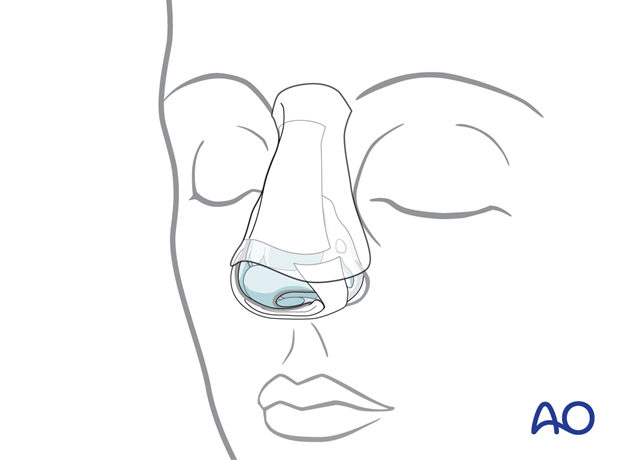
After reduction, adhesive strips are placed over the skin of the nasal dorsum, and the nasal bones are splinted using an external splint that conforms to the patient’s nose. If the nasal bones are comminuted or loose, they should be supported with an intranasal packing, which should be placed before placing the external splint.
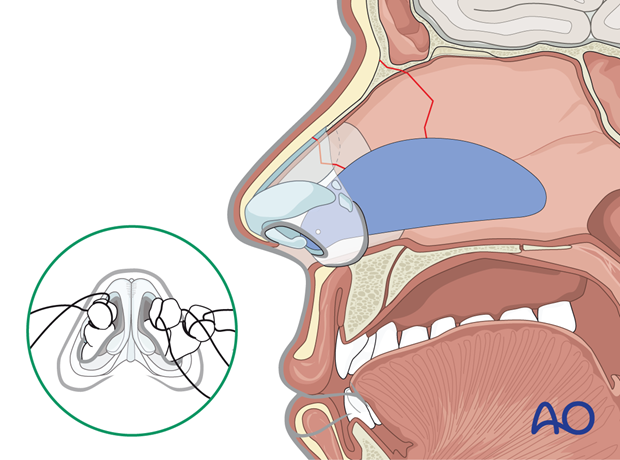
Nasal septum
The nasal septum can be stabilized with splints (Doyle) or packs.
The Doyle splints are made from silicone and are placed on either side of the septum, secured by one or multiple sutures. They are designed to prevent the formation of a septal hematoma, splint septal cartilage, and maintain an open airway.
Removal of packings and splints
Hemostatic packs are removed after 24 hours. Packs supporting the nasal bones are left in place as long as the external splint is in place. They can be left in place anywhere from 5 to 10 days).
The patient should be prescribed antibiotic treatment for as long as the nasal packs are in place.
4. Aftercare
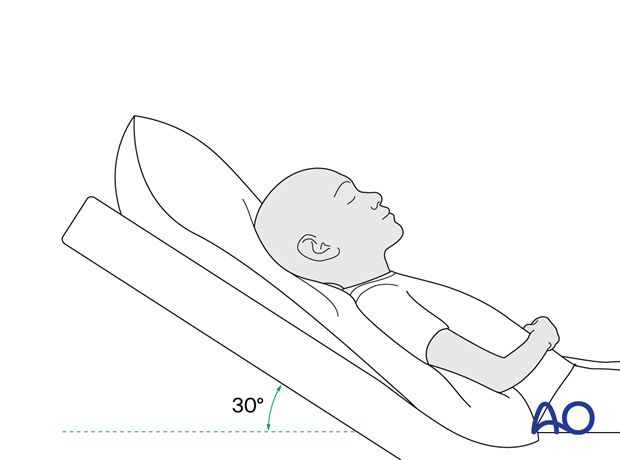
Postoperative positioning
Keeping the patient’s head in a raised position both preoperatively and postoperatively may significantly improve edema and pain.
Nose blowing
Nose blowing should be avoided for at least ten days following nasal fracture repair to prevent orbital emphysema.
Medication
The use of the following perioperative medication is controversial. There is little evidence to make solid recommendations for postoperative care.
- No aspirin prescribed for seven days (nonsteroidal anti-inflammatory drugs (NSAIDs) use is controversial).
- Provide analgesia as necessary.
- Antibiotics (Many surgeons use perioperative antibiotics. There is no clear advantage of any antibiotic, and the recommended duration of treatment is debatable.) More information can be found in the article: Mundinger GS, Borsuk DE, Okhah Z, et al. Antibiotics and facial fractures: evidence-based recommendations compared with experience-based practice. Craniomaxillofac Trauma Reconstr. 2015 Mar;8(1):64-78.)
- A nasal decongestant may be helpful for symptomatic improvement in some patients.
Postoperative imaging
For nasal fractures, postoperative CT imaging is usually not necessary.
Wound care
Ice packs may be effective in the short term to minimize edema.
Avoid sun exposure and tanning to skin incisions for several months.
Diet
Diet depends on the fracture pattern and the patient’s condition, but there are usually no limitations.
Clinical follow-up
Clinical follow-up depends on the complexity of the surgery and the patient’s postoperative course.
In all patients with nasal bone trauma, all the following should be periodically assessed:
- Nasal airway status
- Excess compression from the splint or intranasal material
- External nasal deformity
- Other issues to consider are:
- Facial deformity (incl. asymmetry)
- Sensory nerve compromise
- Problems of scar formation
- Anosmia
- Epiphora and dacryocystitis













