Posteromedial approach to the talus
1. Introduction
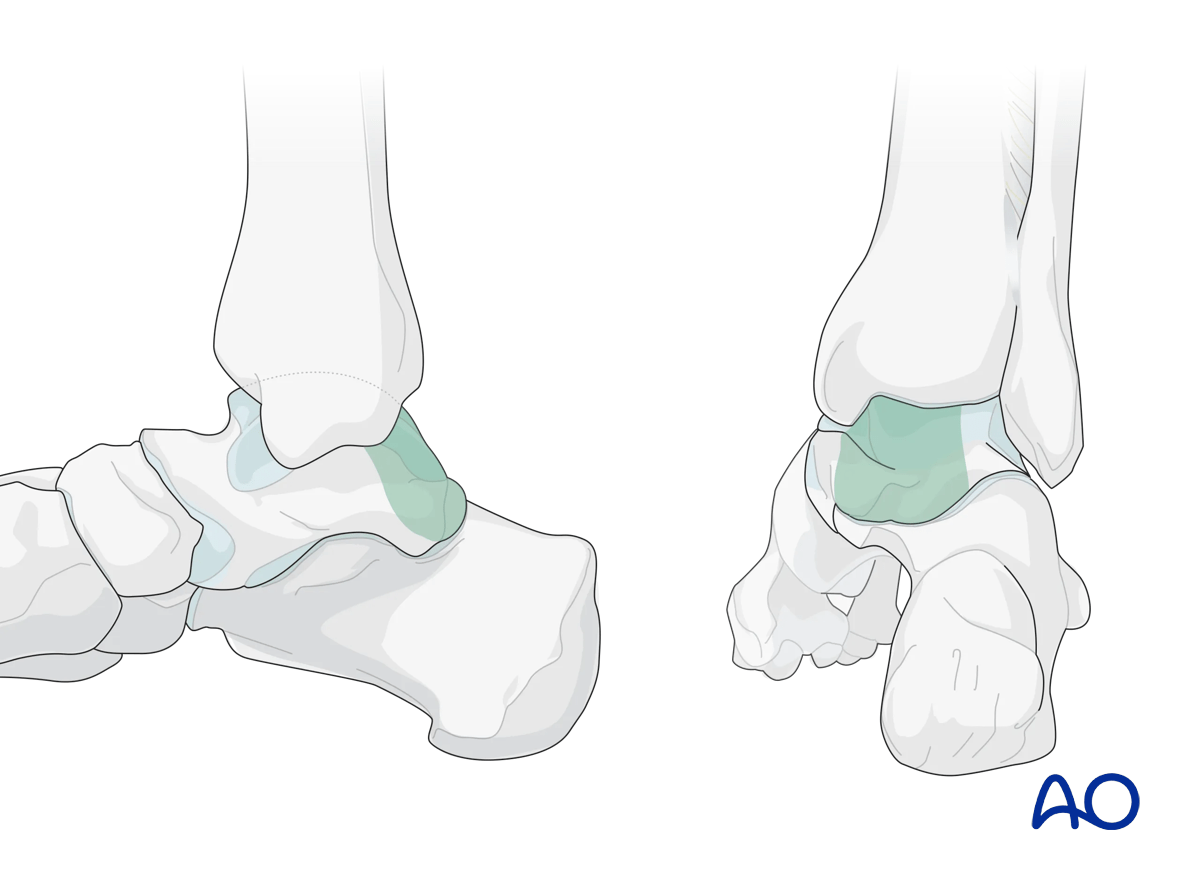
This approach is utilized for posteromedial fractures of the talar body or posterior process fractures of the talus but would not give visualization of the anterior half of the talar body. Only the posterior aspects of the tibiotalar and posterior talocalcaneal joint may be visualized with this approach.
This illustration shows the area of the talus that are visualized through this surgical approach.
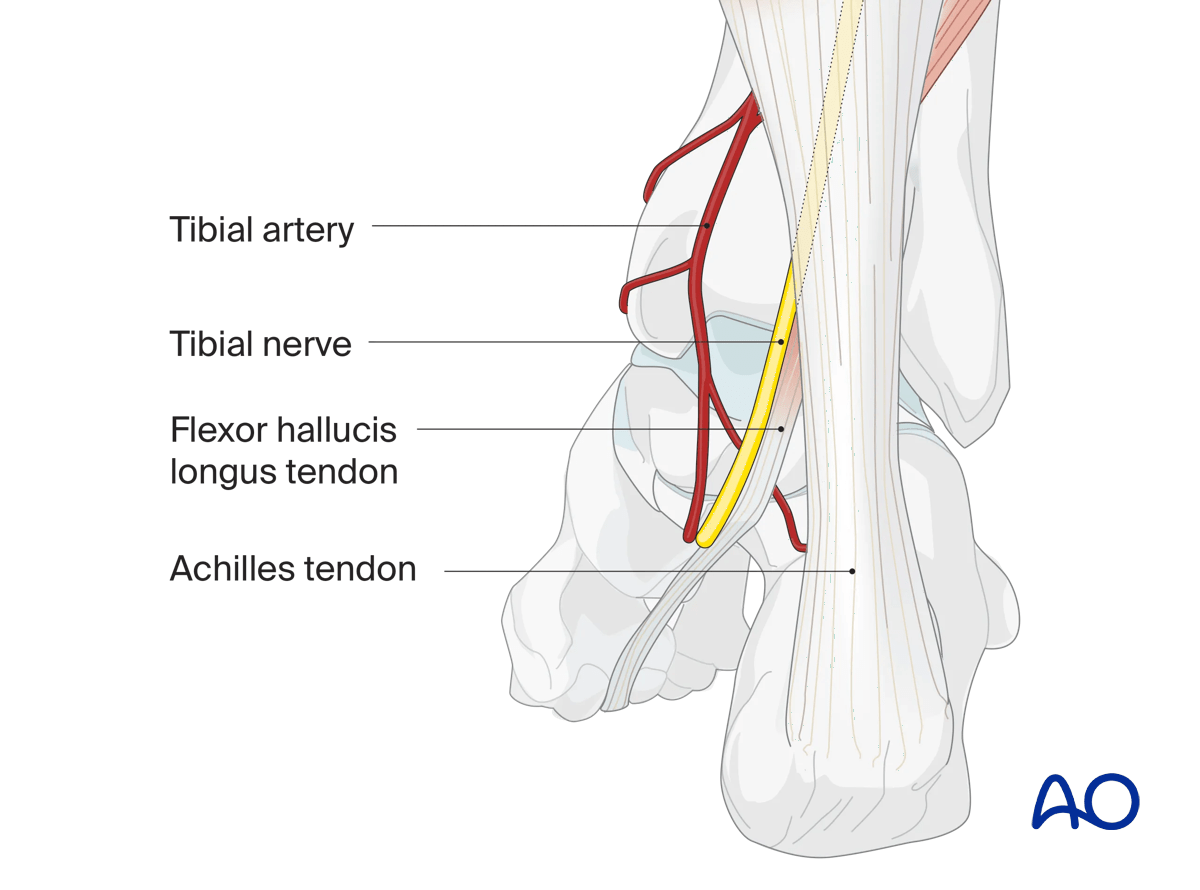
2. Anatomy
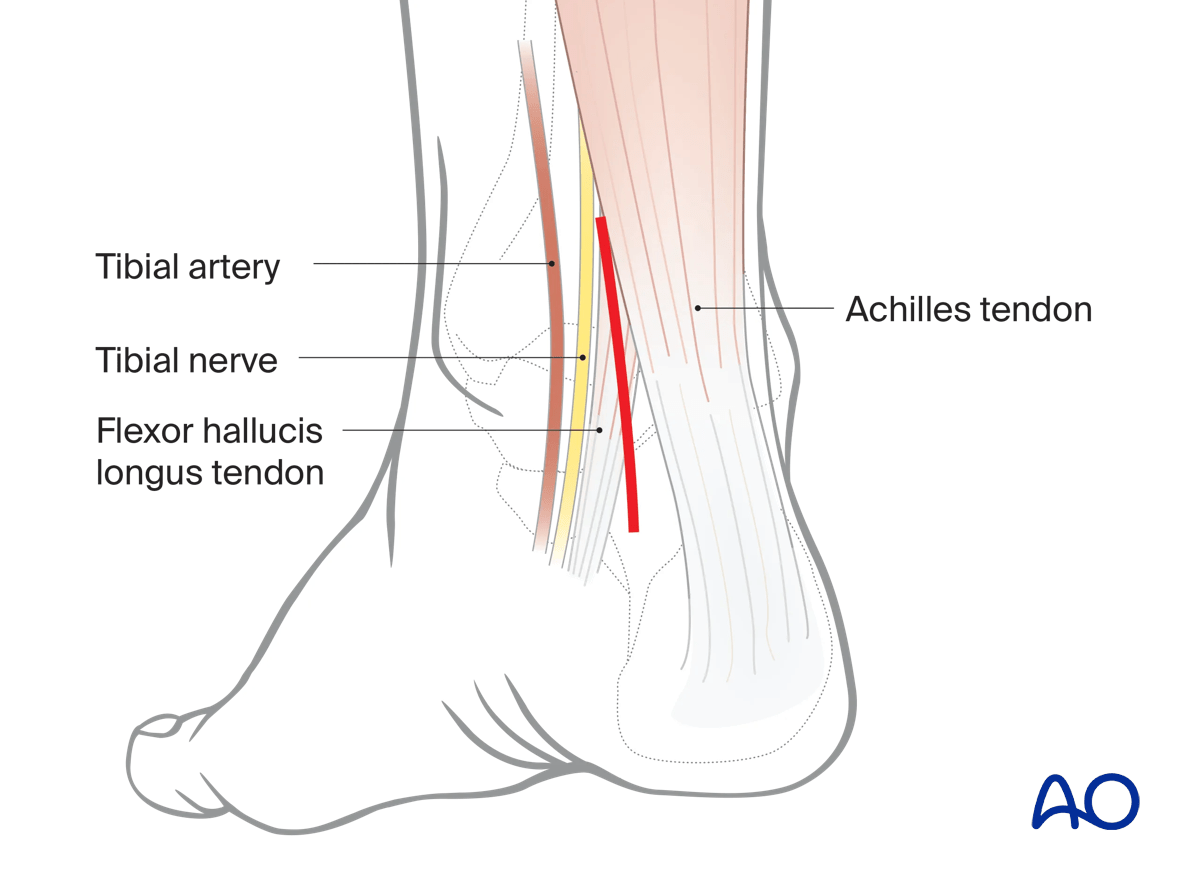
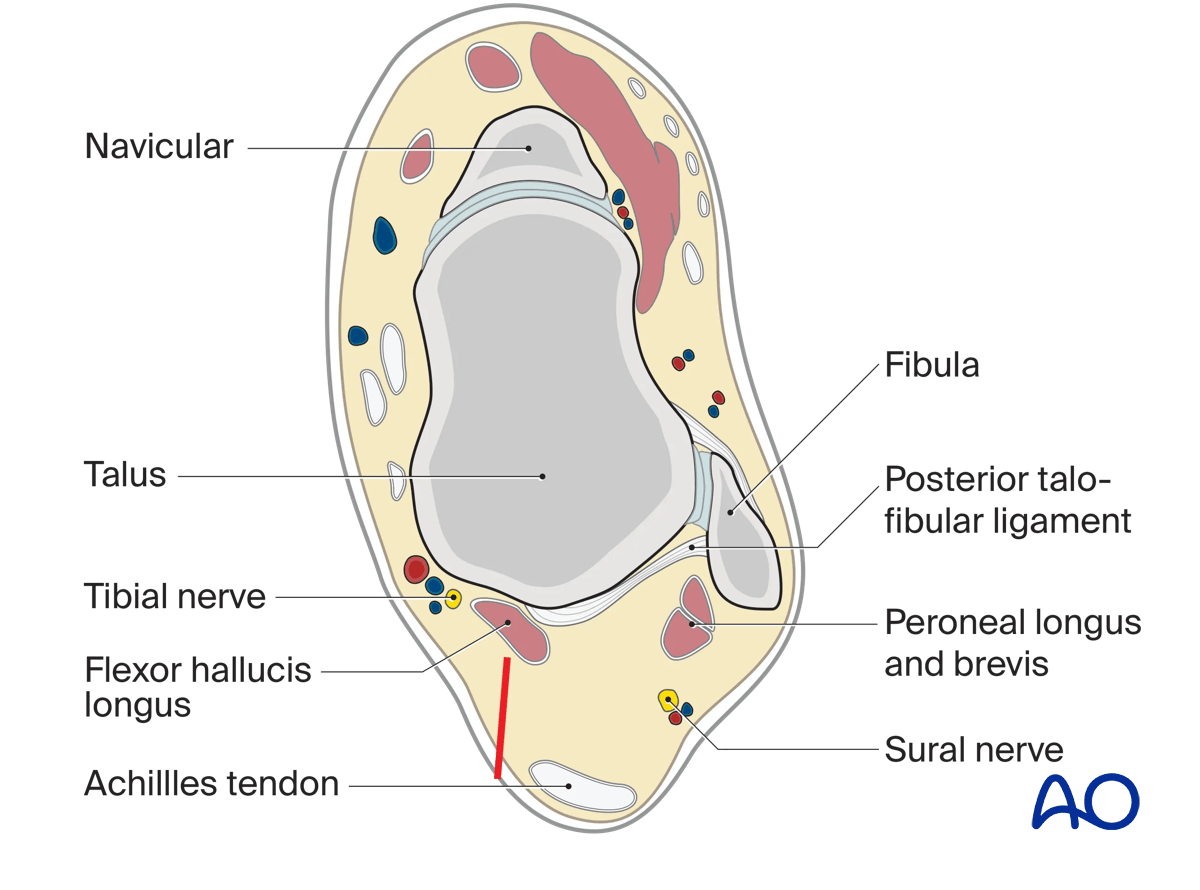
The approach follows the plane between flexor hallucis longus (FHL) and the medial border of the Achilles tendon.
The neurovascular structures lie directly in this approach behind the medial malleolus and must be protected.
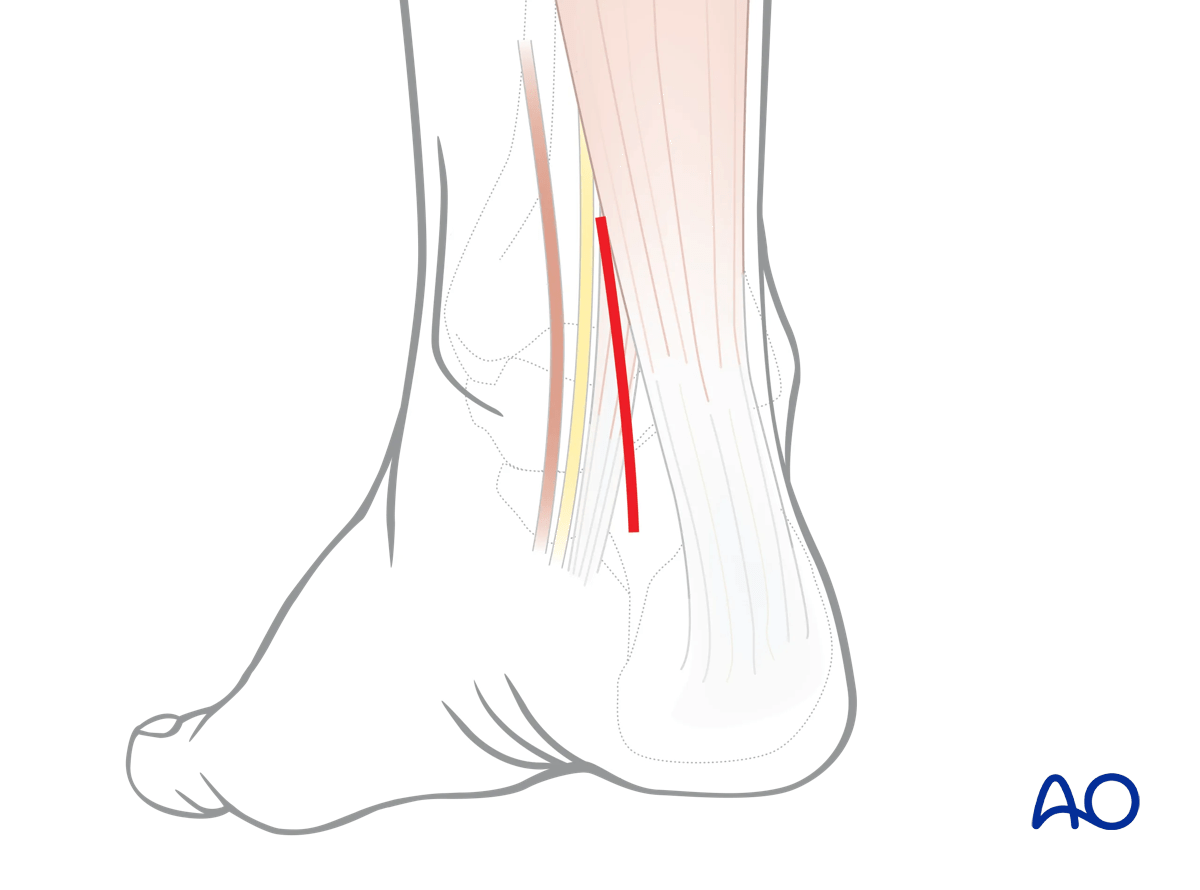
3. Incision
The skin incision is between the Achilles tendon laterally and the medial malleolus medially.
The precise position of the incision depends on the anatomy.
Perform a skin incision centered over the subtalar joint. An image intensifier may be used as a guide.
Identify the FHL tendon, the most posterior structure. Dissect posterior and laterally, medial to the Achilles tendon.
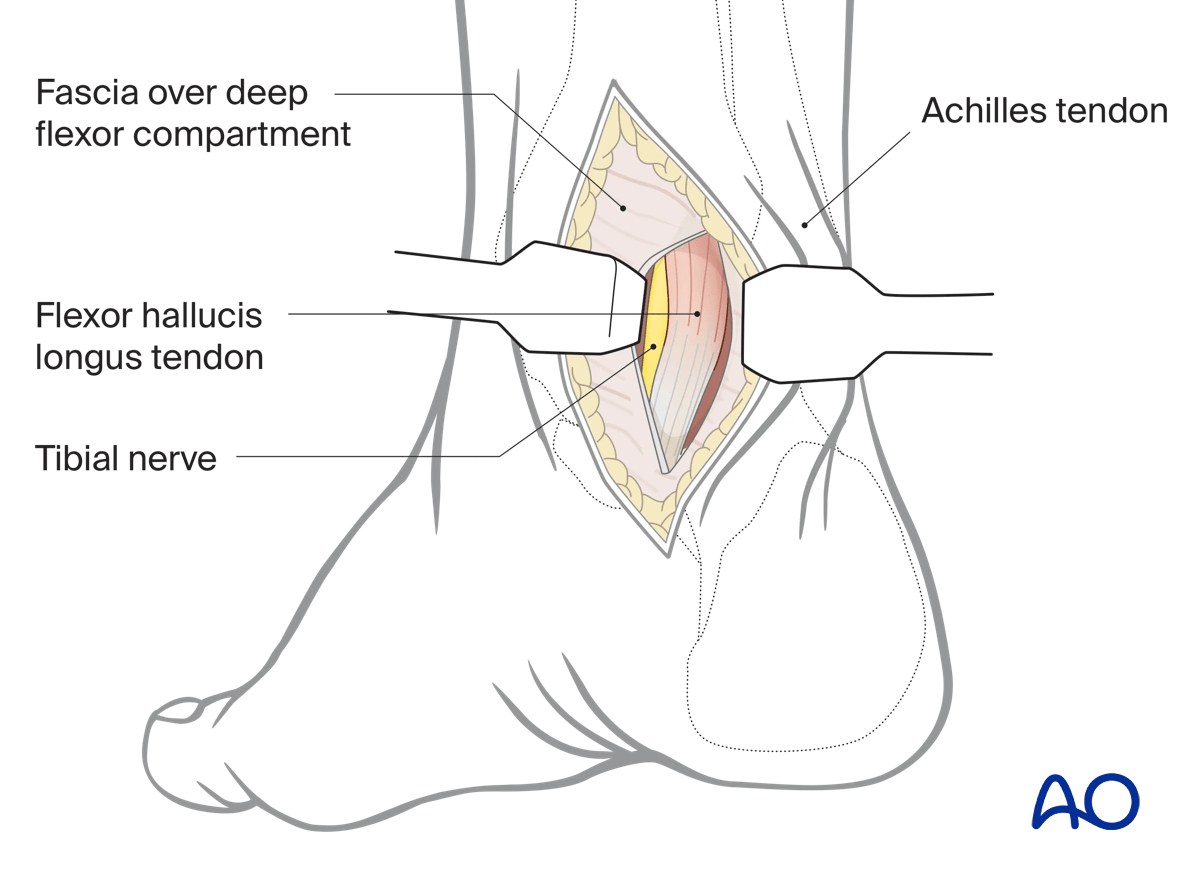
Deep dissection
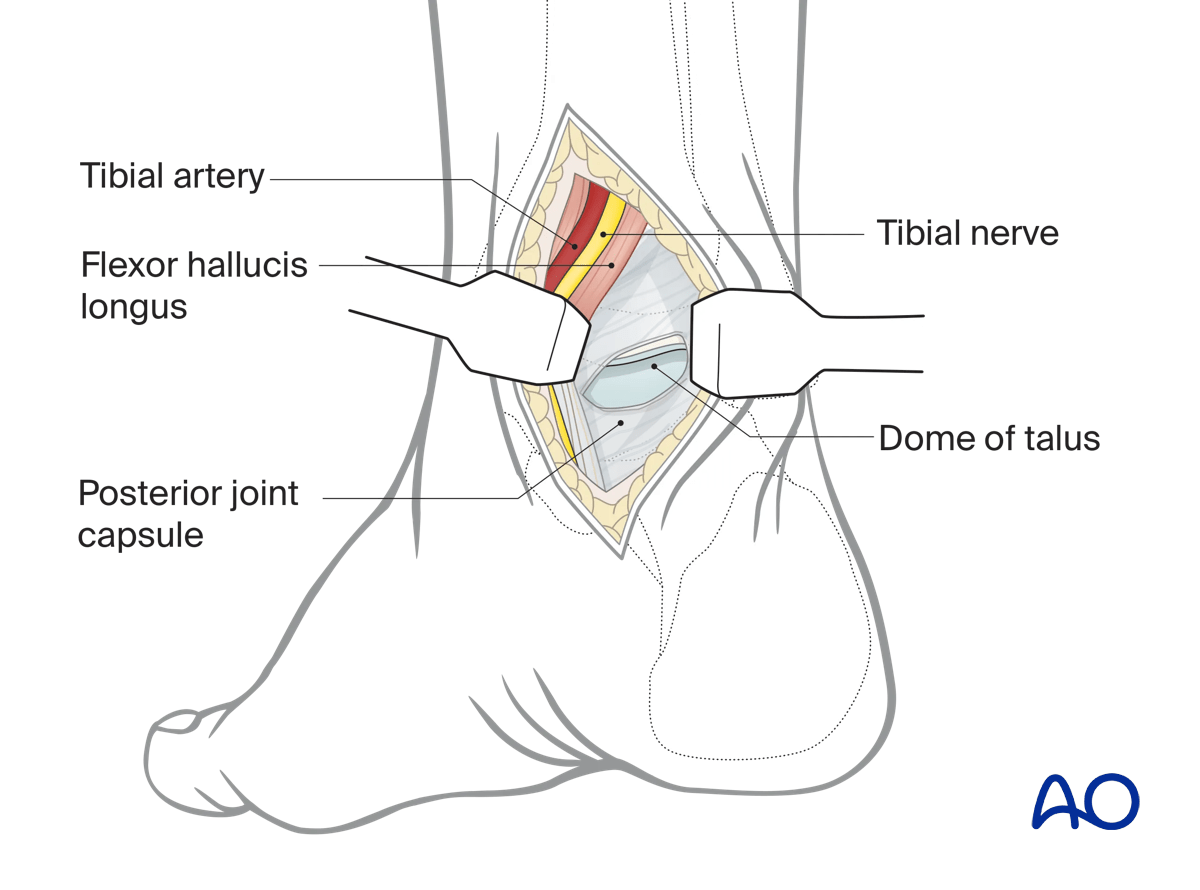
Deepen the dissection lateral to the FHL and, if necessary, open its tendon sheath. This allows the retraction of the tendon together with the neurovascular bundle and gains exposure to the fracture.
The FHL travels between two tubercles on the posterior talar body. Fractures may occur through the intertubercle groove, and the FHL may be used to help identify the reduction of displaced fracture fragments.
Fracture debridement, reduction, and fixation can now be completed.
An external fixator or distractor between the distal tibia and calcaneus may be used to assist exposure to the talus.
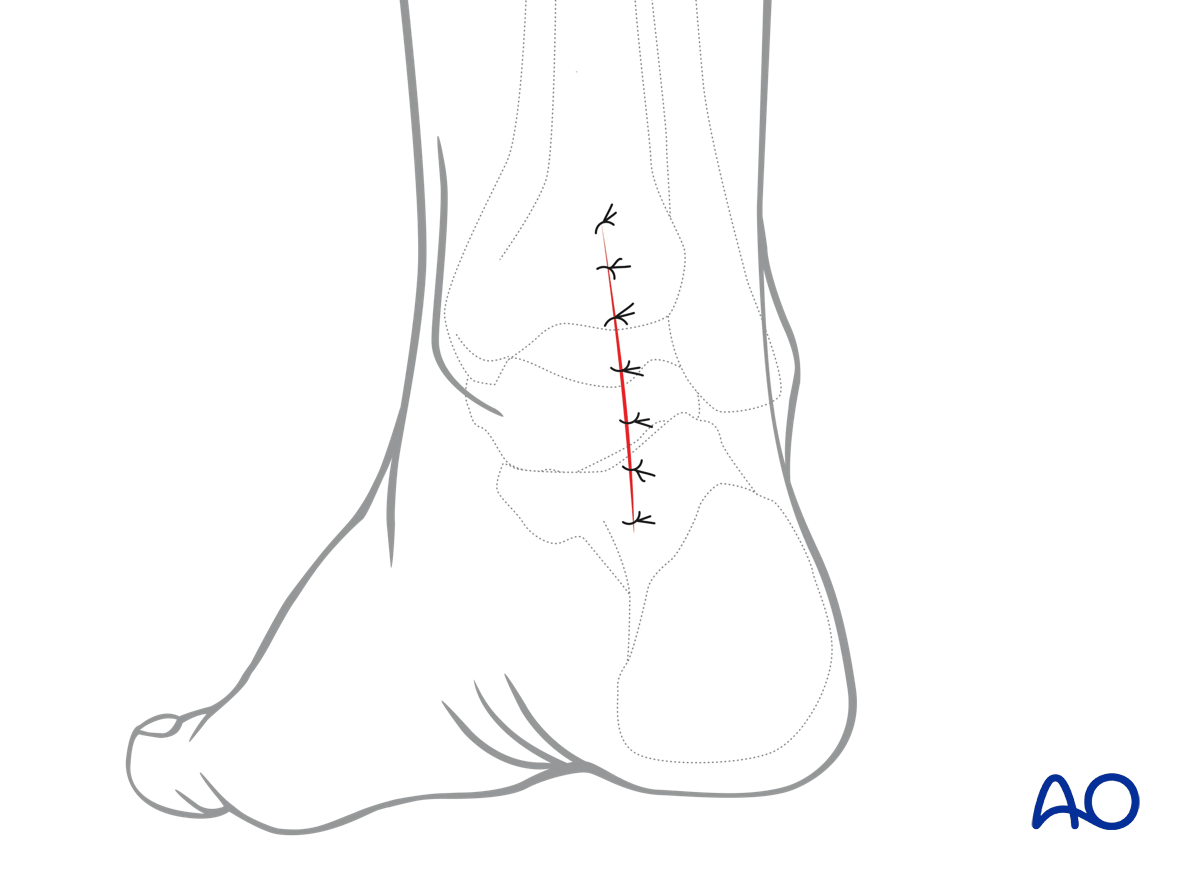
4. Wound closure
This approach is closed in layers reconstructing all the deep structures and avoiding compromise of the posterior tibial neurovascular bundle.