Posterolateral approach to the hindfoot
1. Introduction
The posterolateral approach provides access to the posterior half or the talar body and can be used for acute posterior talar fractures and nonunion surgery. It can also be used for posterior stabilization of a talar neck fracture after reduction.
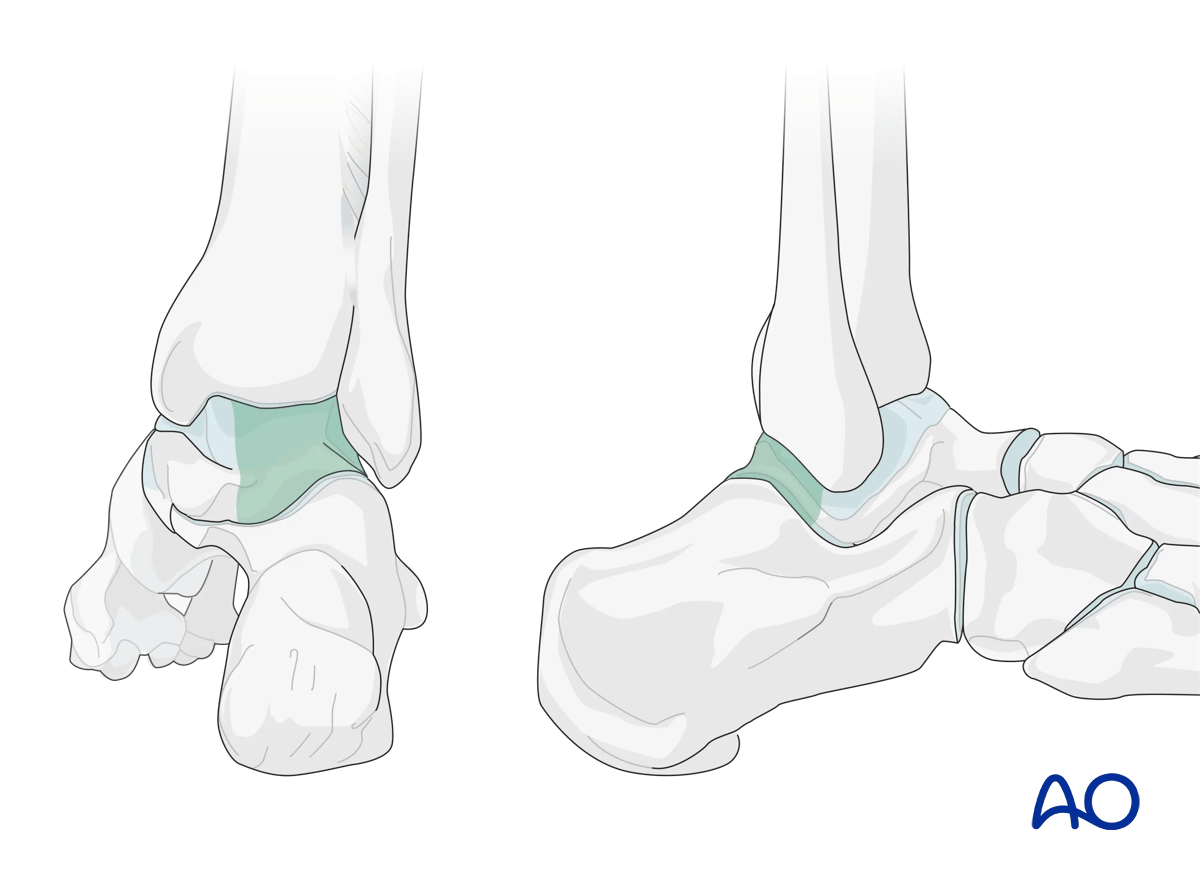
This approach exposes the posterior talus, the posterior aspect of the distal tibia, the posterior distal fibula, and the posterior portion of the calcaneus.
The incision involves the vertical limb of the extended lateral approach to the calcaneus. It may be extended more distally and proximally compared with the vertical limb of a typical extended lateral approach.
The advantage compared to the posteromedial approach is that it is not putting to risk the neurovascular bundle. The disadvantage is it is a very deep dissection to expose the back of the talus, and proximally the approach is not extensile because of the flexor hallucis longus (FHL).
This illustration shows the areas of the talus that are visualized through this surgical approach.
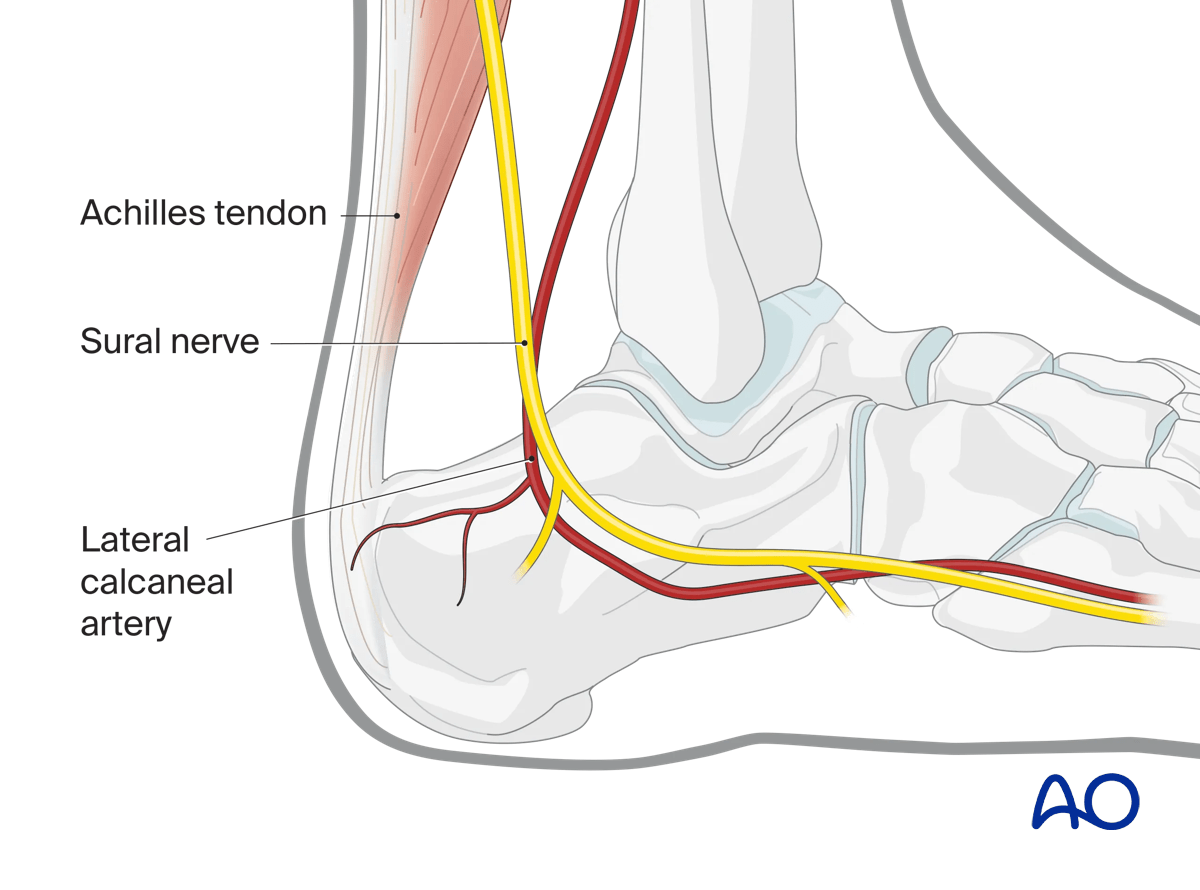
2. Anatomy
The lateral calcaneal artery is responsible for most of the blood supply to this area.
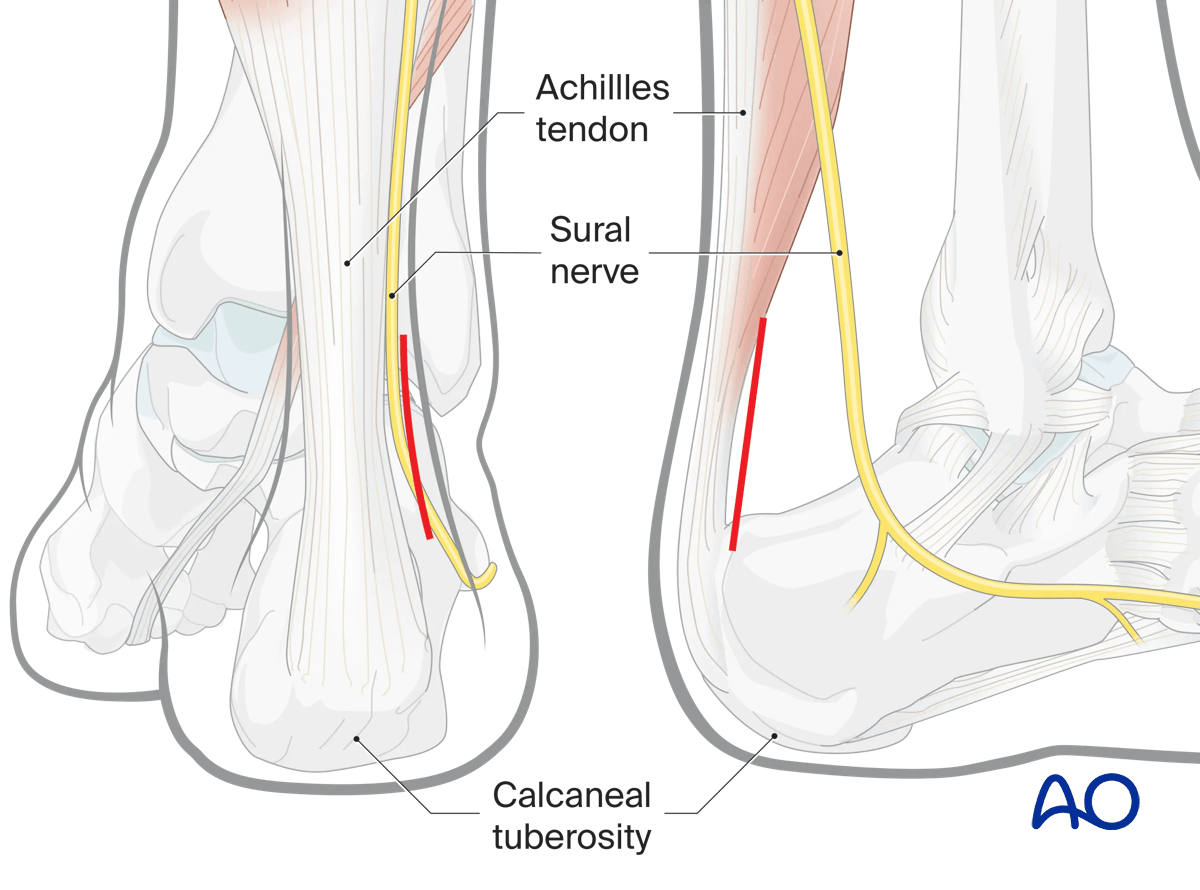
This approach respects the Achilles tendon, sural nerve, and lateral calcaneal artery (posterior peroneal artery).
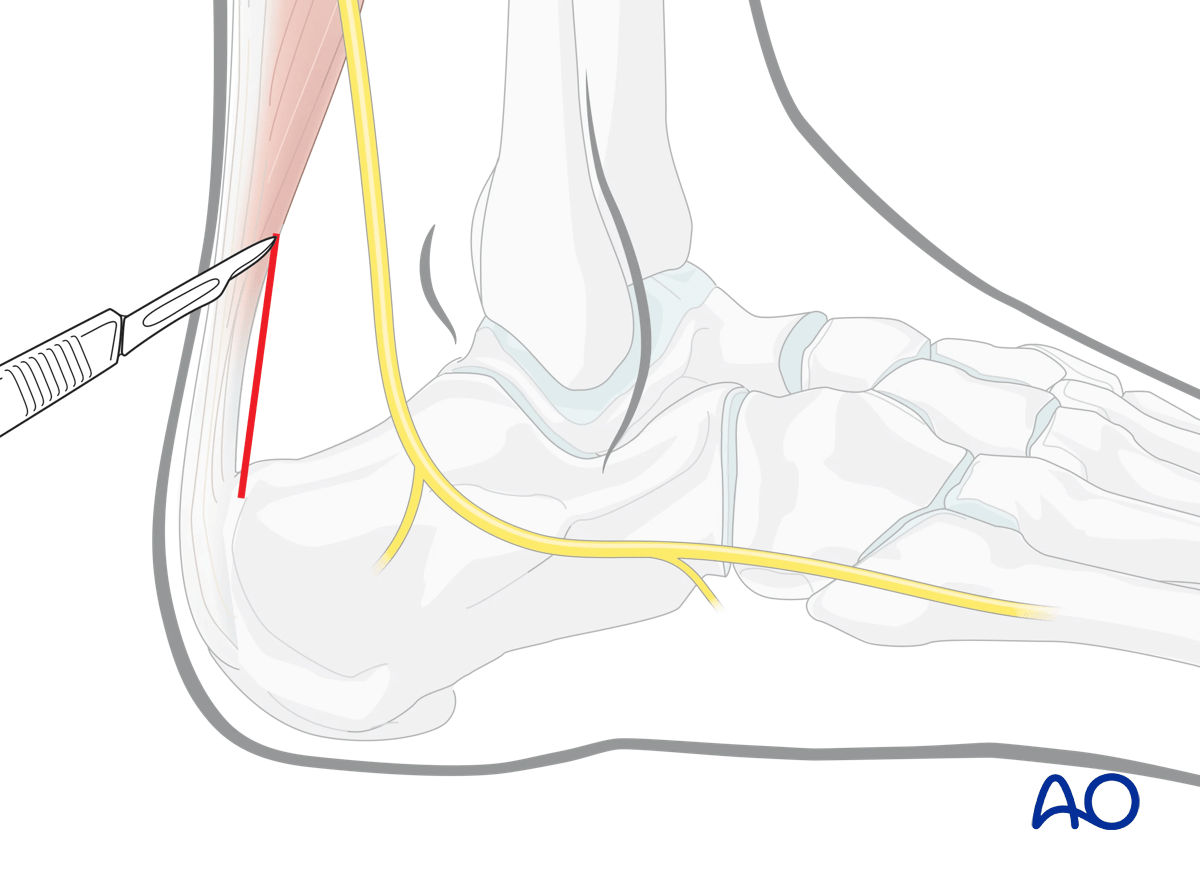
3. Incision
The landmarks for this incision are the lateral aspect of the Achilles tendon and the calcaneal tuberosity. The incision should not be over the Achilles tendon.
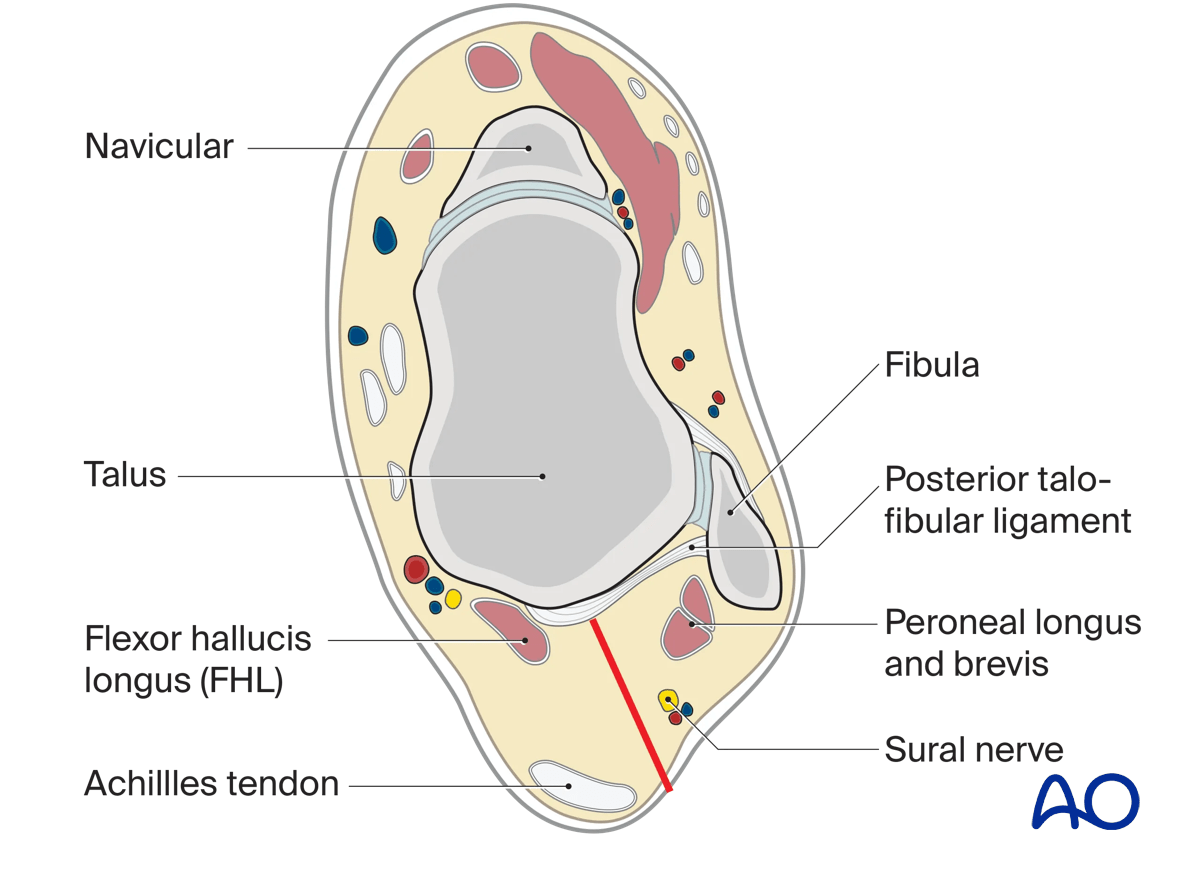
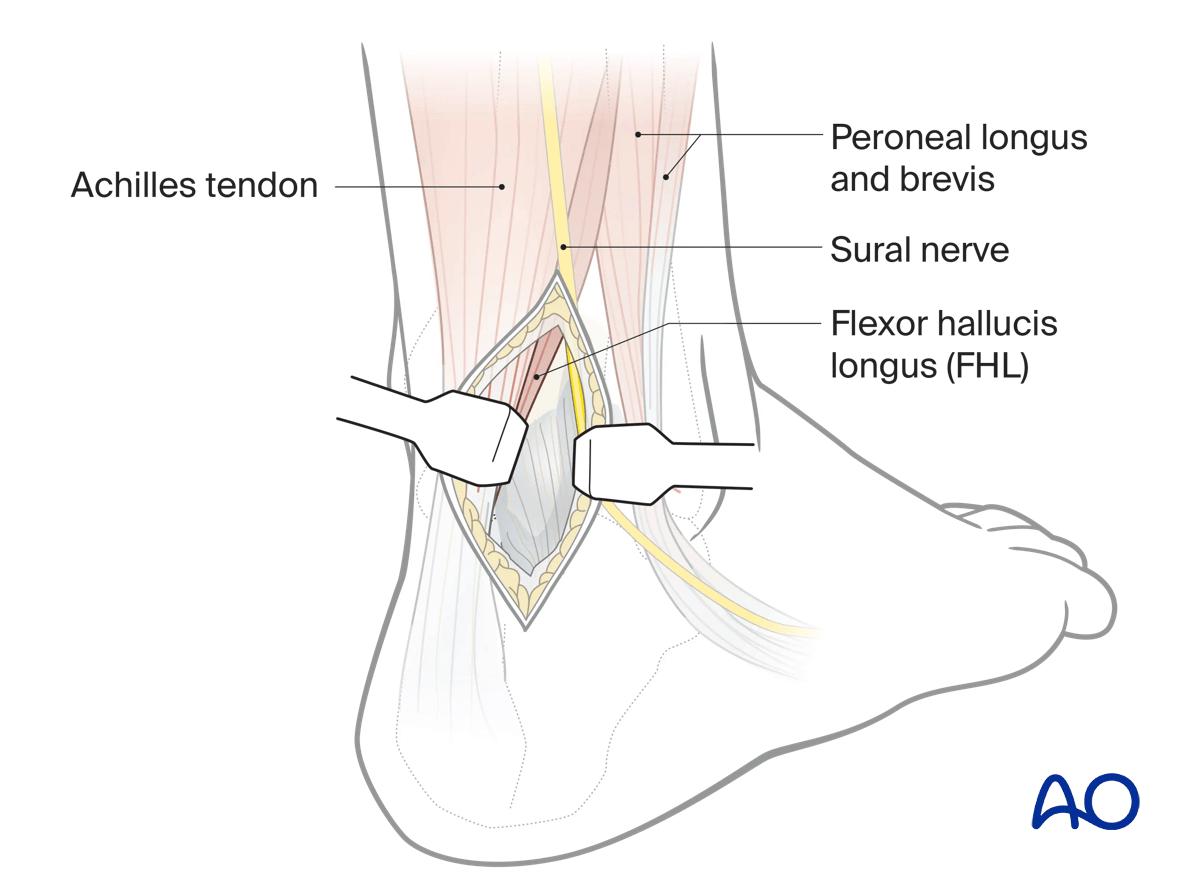
Deepen the incision lateral to the paratenon of the Achilles tendon, then through the fat of the pre-Achilles space.
Medially, the belly of FHL protects the posterior tibial neurovascular bundle.
Incise the capsules of the ankle and subtalar joint vertically. This will expose superiorly the distal tibia and inferiorly the calcaneus with the talar body between them.
The use of a distractor between the tibia and the calcaneum will increase the exposure.
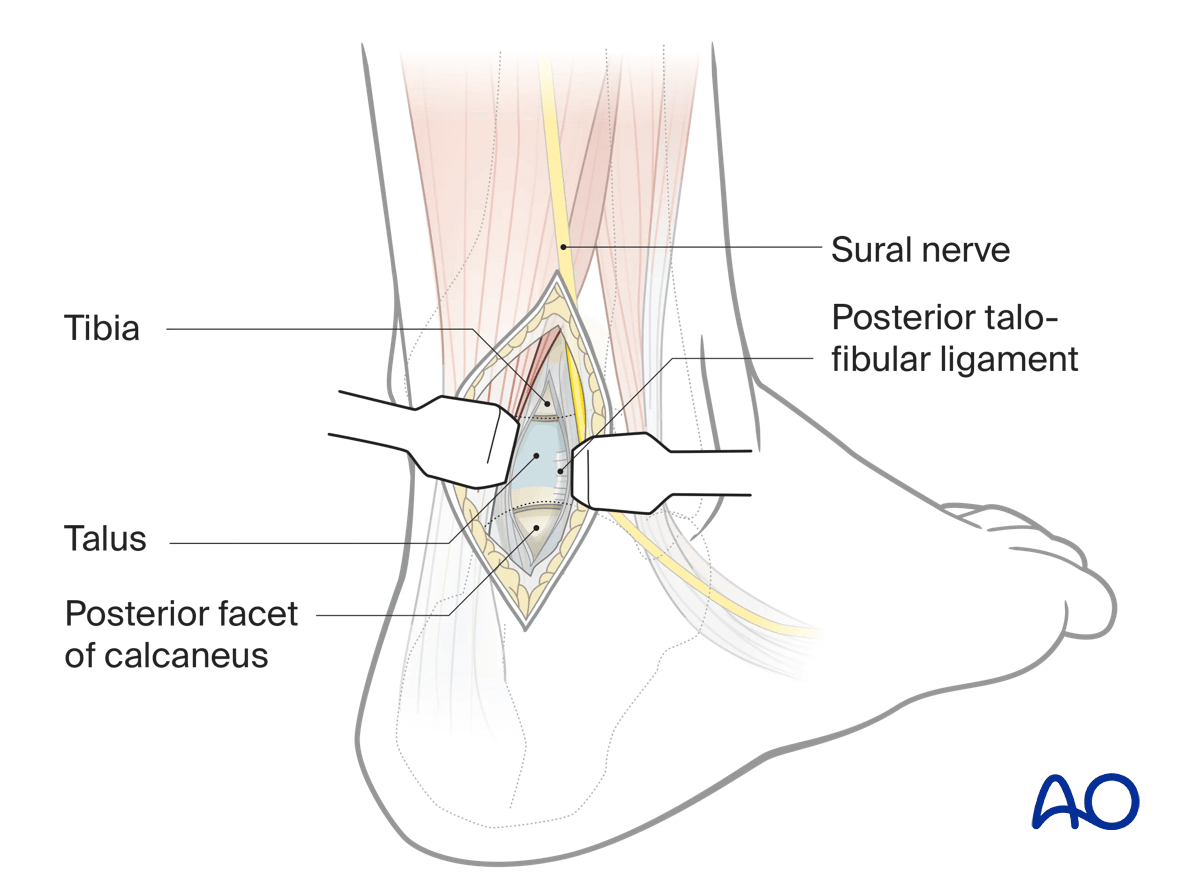
An external fixator or distractor between the distal tibia and calcaneus may be used to assist exposure to the talus.
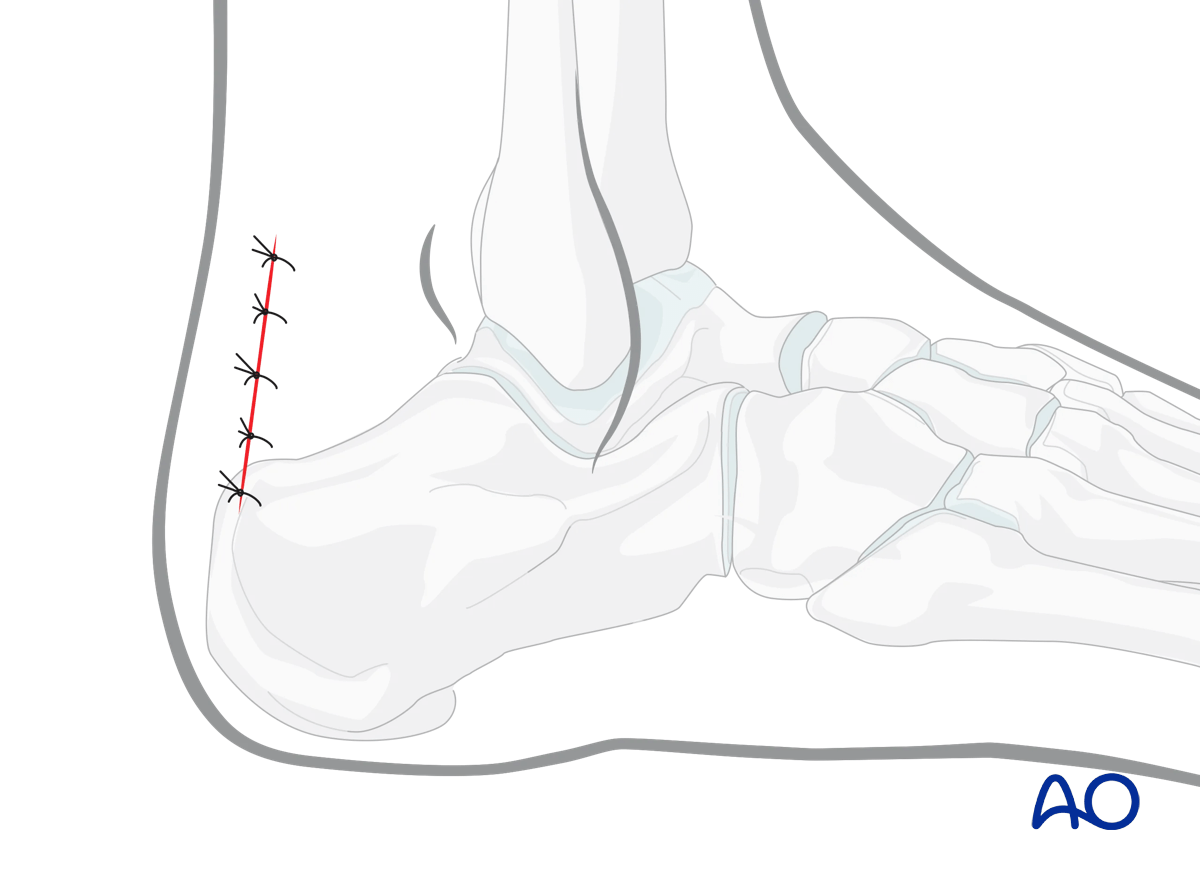
4. Wound closure
This approach is closed in layers.