Lateral malleolar osteotomy
1. Introduction
In uncommon cases, a lateral malleolar osteotomy may be an alternative to the anterolateral approach for management of posterior and lateral talar body fractures.
Similar to the medial malleolar osteotomy, this lateral approach allows reflection of a bony structure and provides much better visualization of an anatomic area which one can not reach otherwise.
The extent of iatrogenic trauma to bone and soft tissue with this approach must be weighed against its potential benefits in fracture visualization.
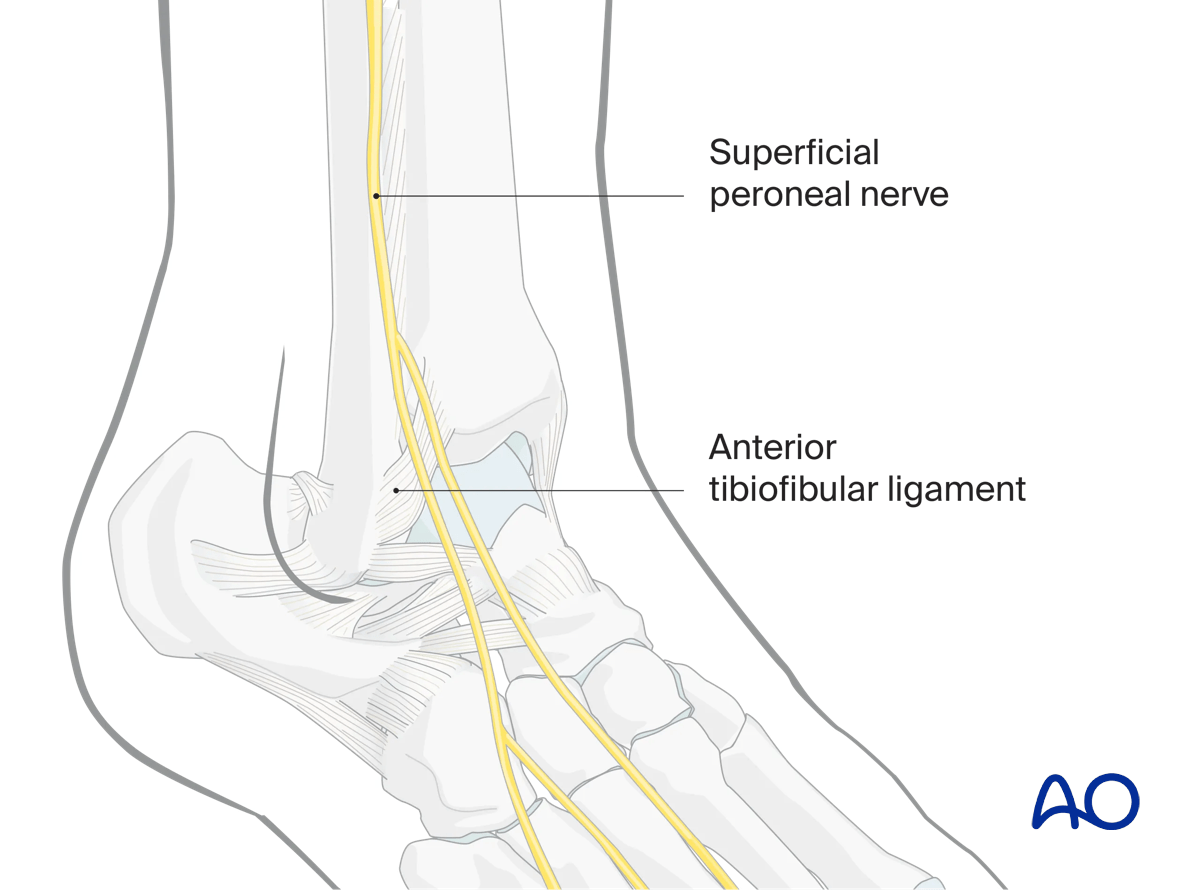
2. Anatomy
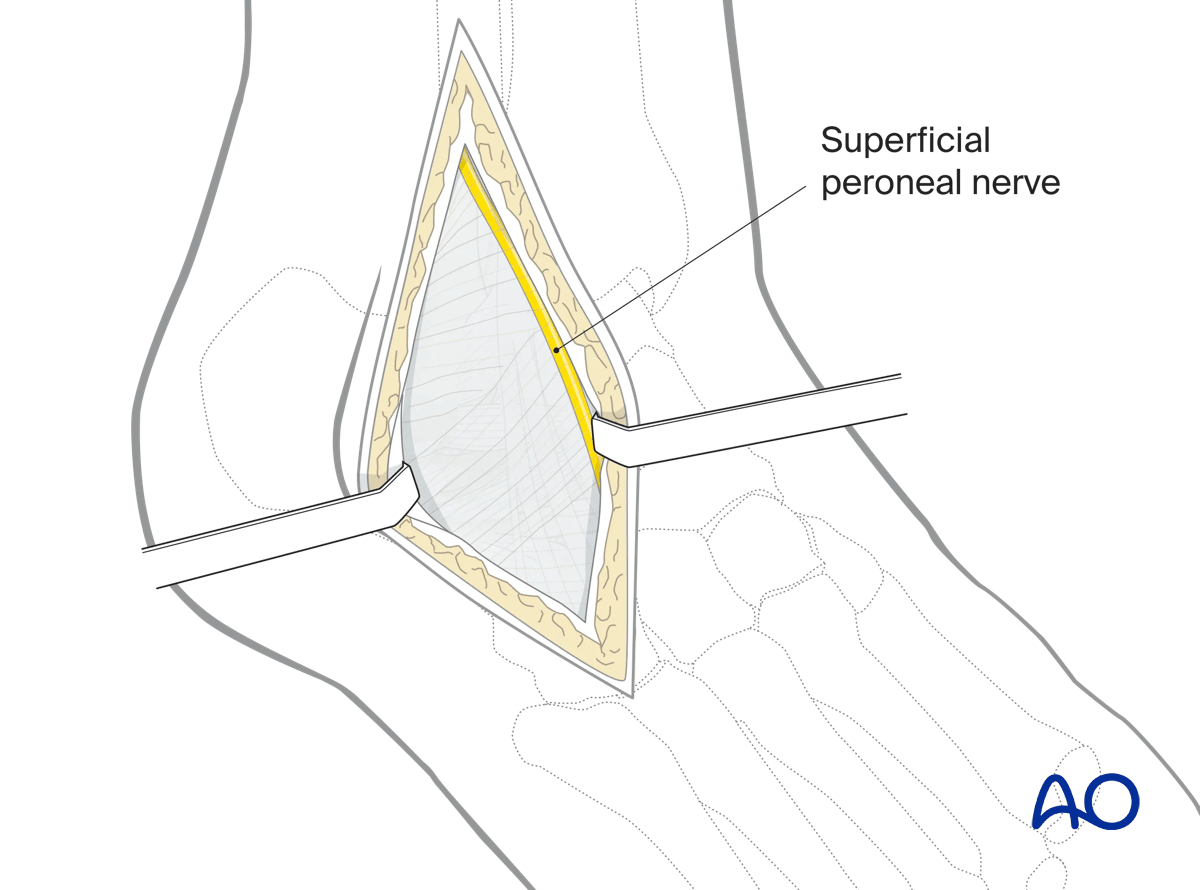
Immediately anterior to the fibula lies the superficial branch of the peroneal nerve. Its location is variable and must be protected with this approach.
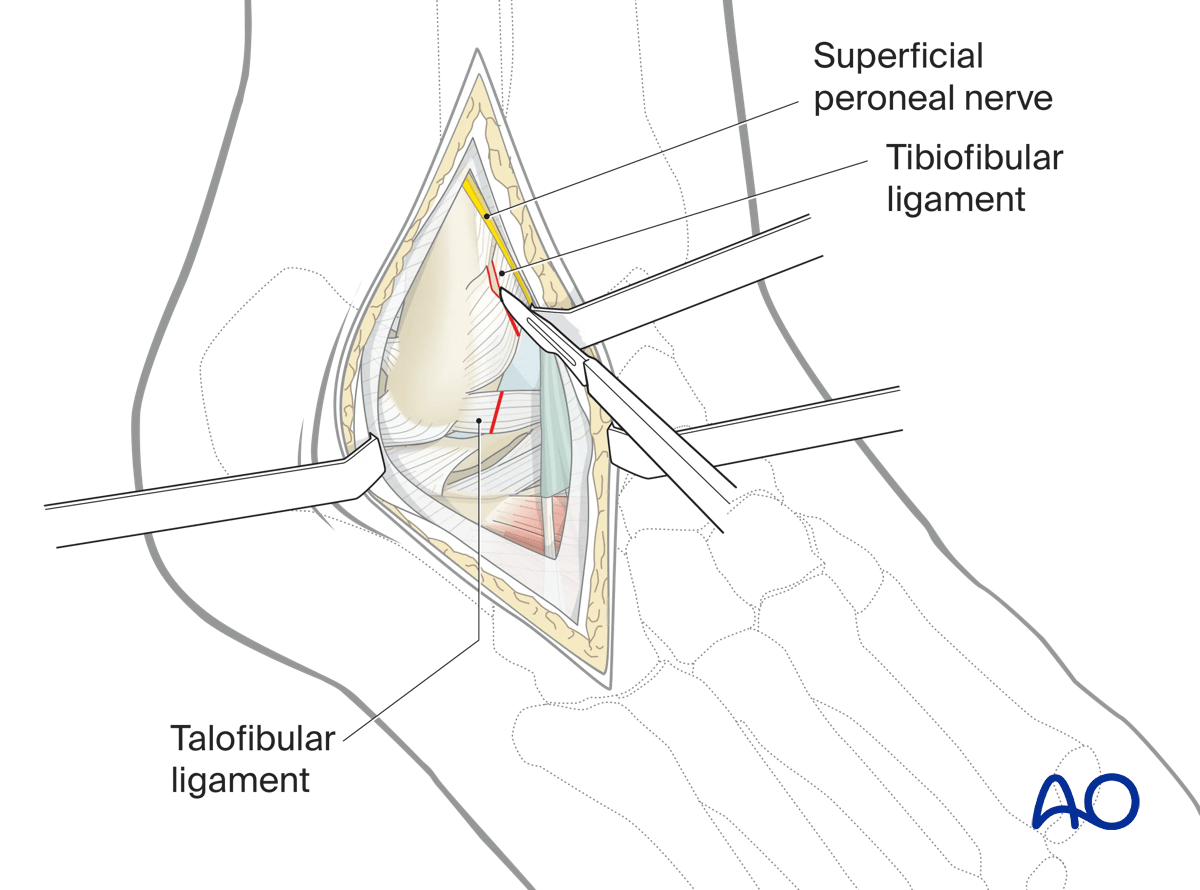
The anterior distal tibiofibular and talofibular ligaments must be divided in this approach. They should be reconstructed at the end of the procedure due to their structural importance. The calcaneofibular ligament is preserved.
The peroneal blood supply is a posterior structure and is not endangered with this approach.
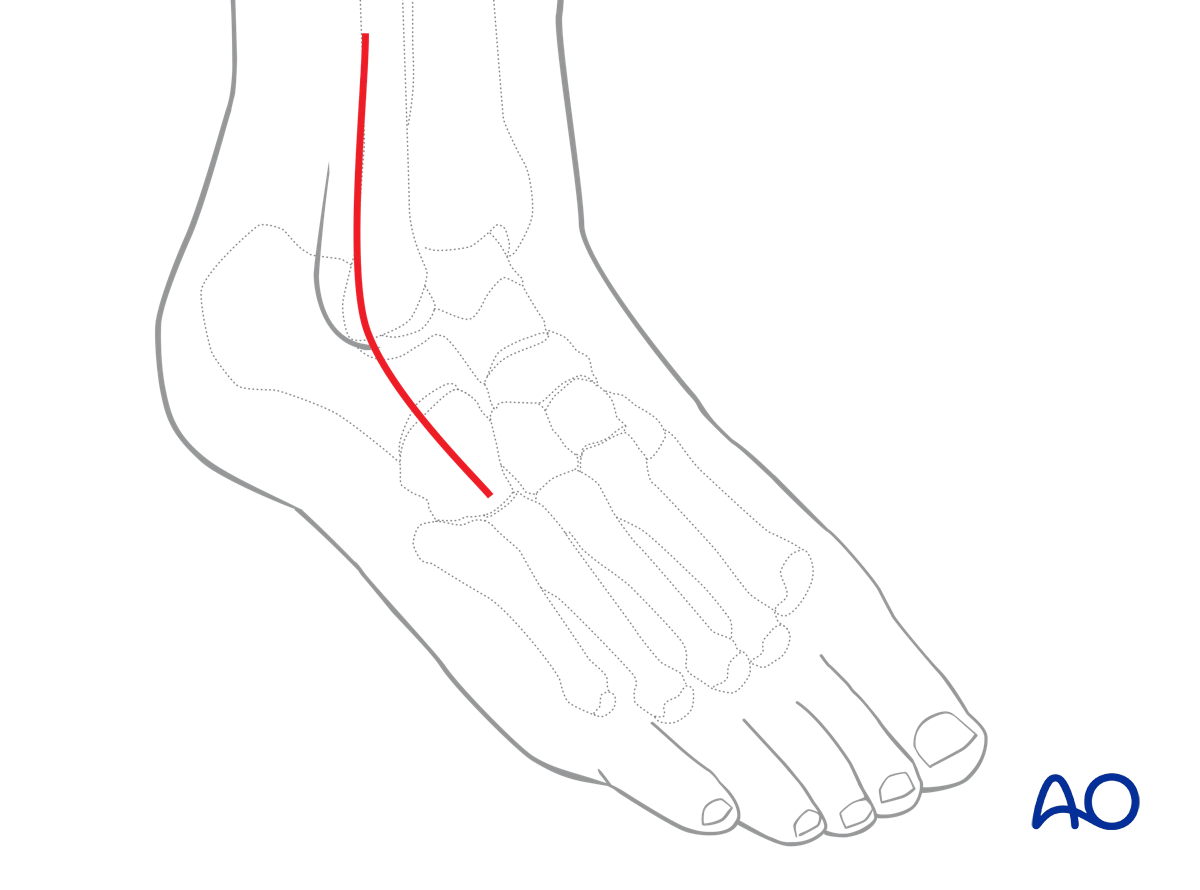
3. Incision
Skin incision
Around the ankle and hindfoot, full-thickness incisions without undermining are imperative. To avoid cutting the branches of the superficial peroneal nerve, the incision must be made longitudinally.
The skin incision is a proximal extension of the anterolateral incision to approach the talus.
Landmarks for this incision are based on the crest of the fibula proximally, down to the tip of the fibula, and then in line with the 4th ray distally.
This skin incision will avoid the superficial peroneal nerve which lies anterior to it.
Deep dissection
Protect the superficial branch of the peroneal nerve carefully. It can either be identified anterior to the incision or avoided by the placement of the incision.
Incise the anterior distal tibiofibular ligament and talofibular ligament.
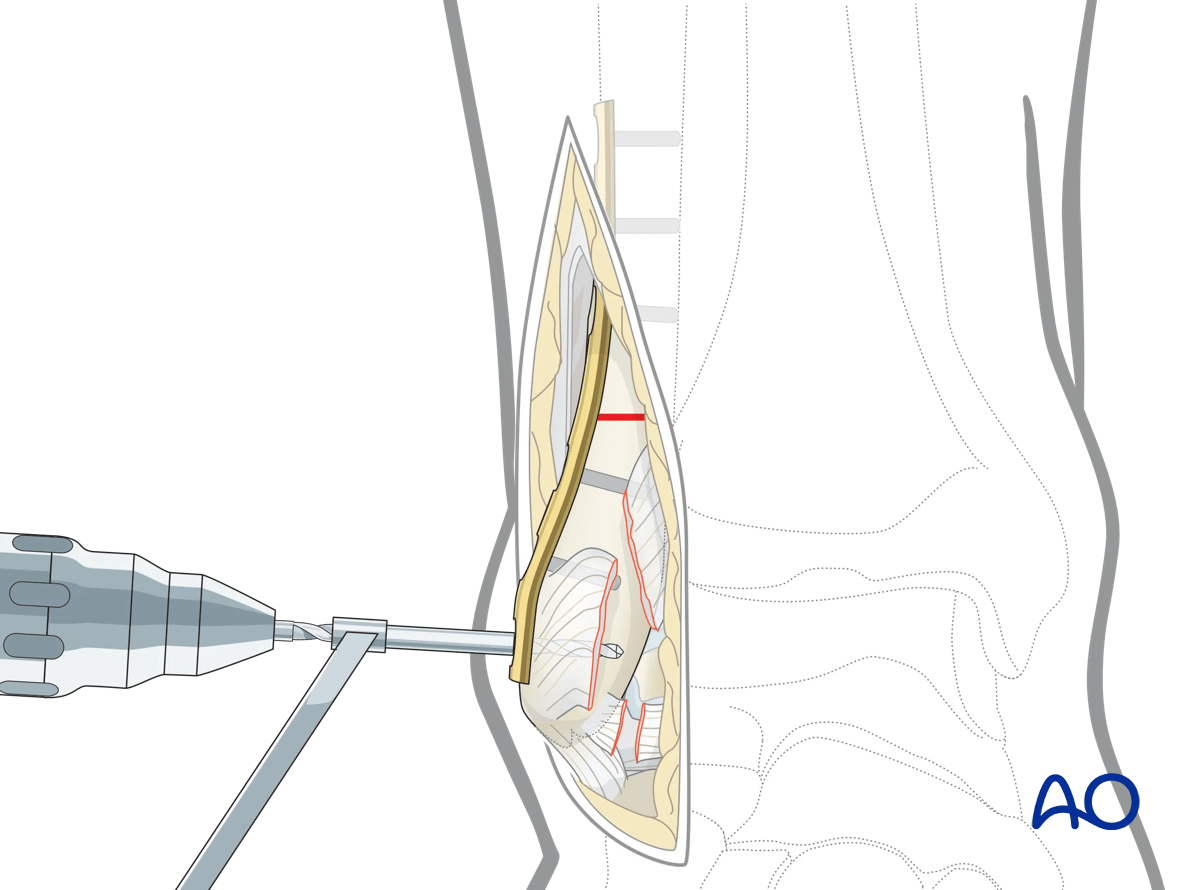
To aid in fibular reduction and fixation after the talus has been fixed, one can consider predrilling holes in the fibula for a plate that will subsequently be used to fix the fibular osteotomy. Care must be taken that the proximal screw holes do not prevent subsequent compression of the osteotomy.
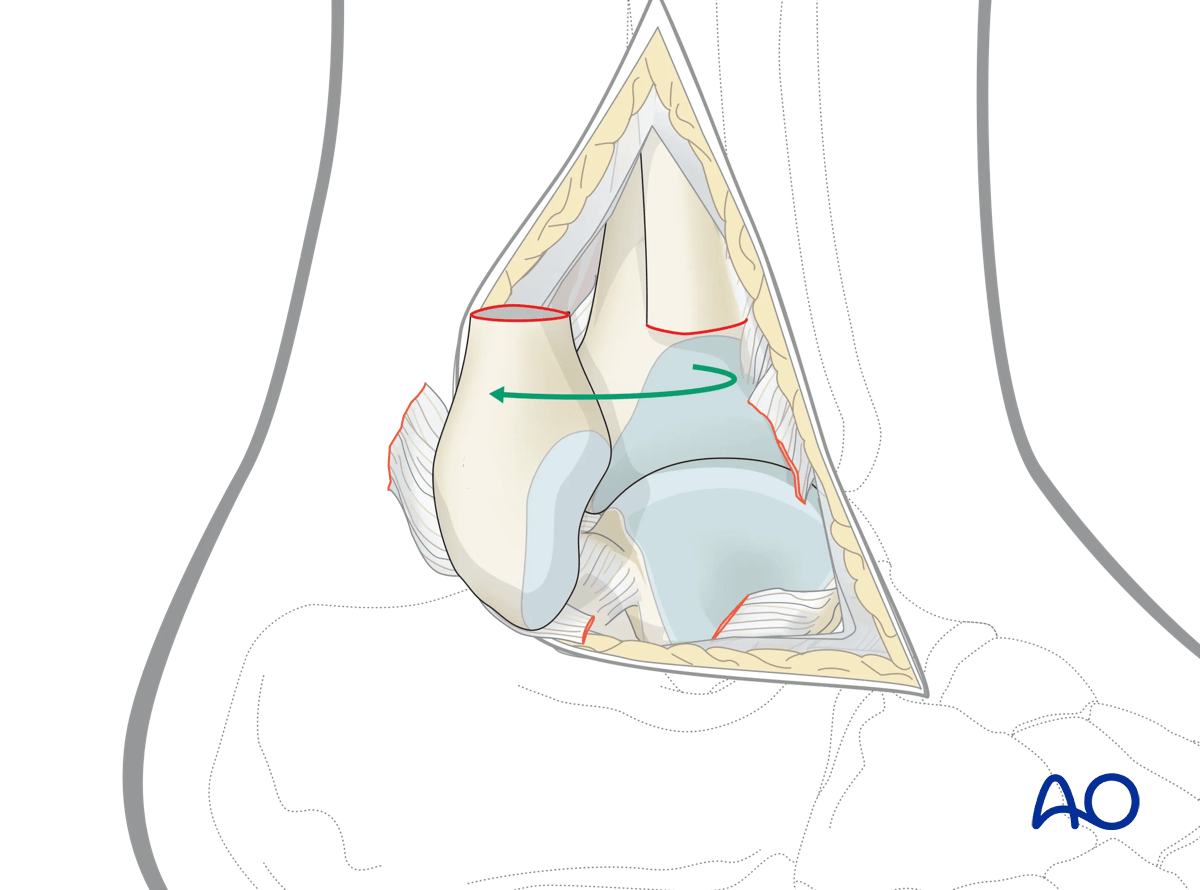
4. Osteotomy
Using image intensification, plan the fibular osteotomy 3 cm above the joint surface, just above the insertion of the distal tibiofibular ligament.
This osteotomy should be transverse to allow compression plating at the end of the procedure. Plan the osteotomy at a level to allow for sufficient fixation of the distal fragment.
Use an oscillating saw.
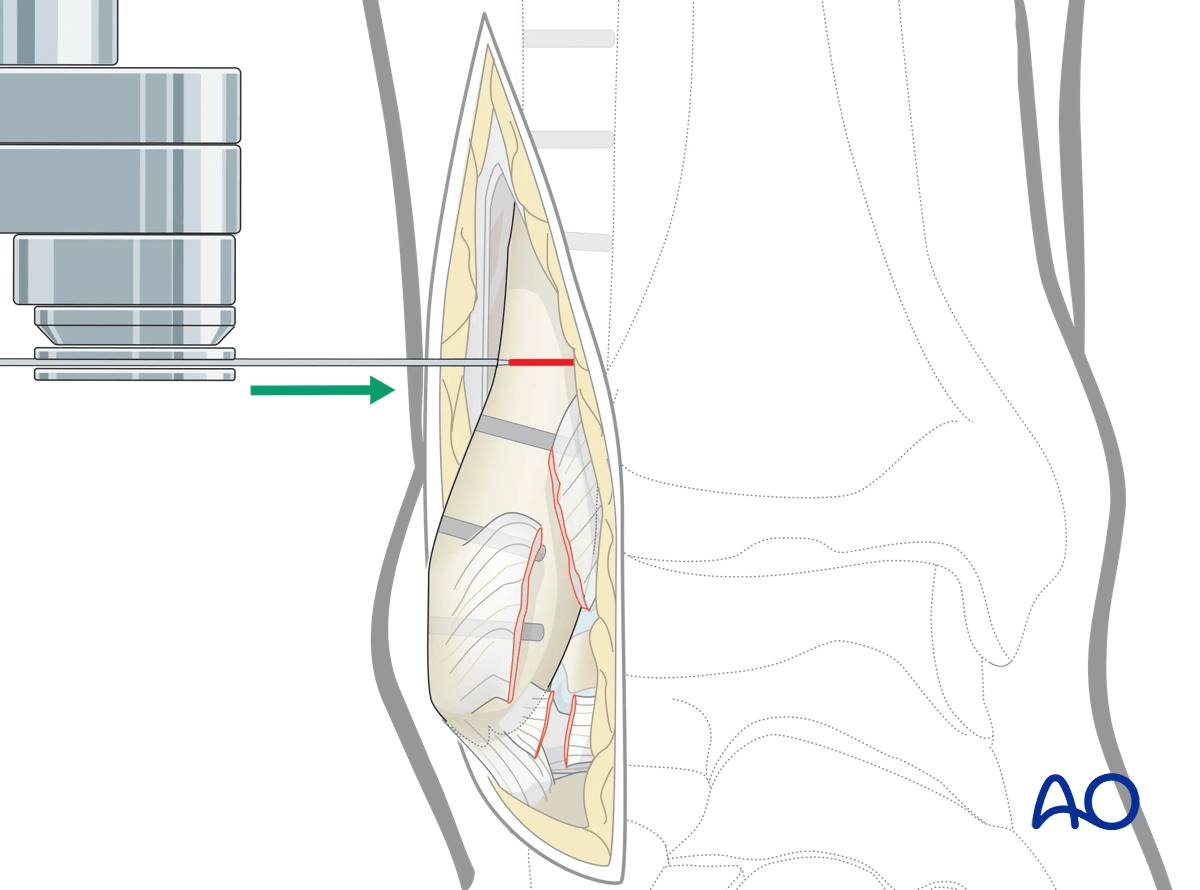
The osteotomy allows the fibula to rotate externally providing excellent visualization of the lateral talus.
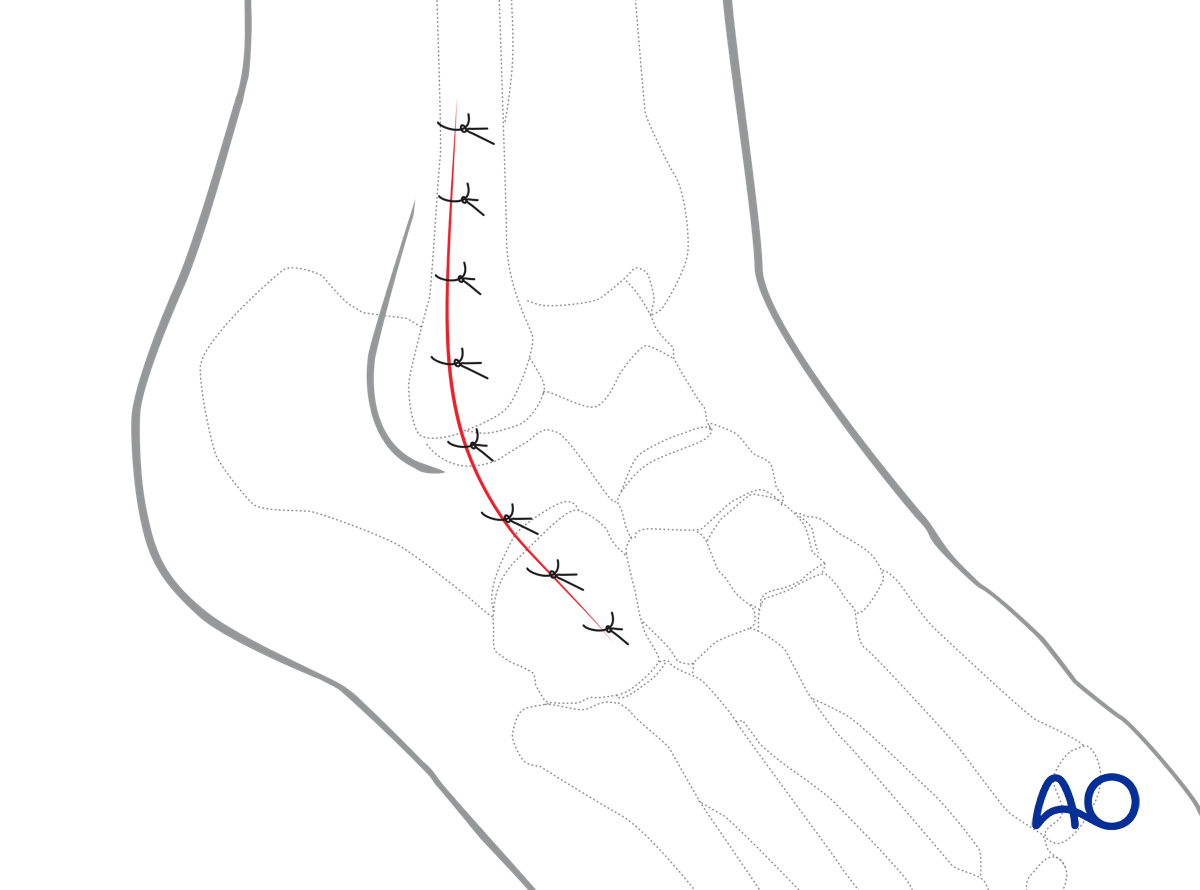
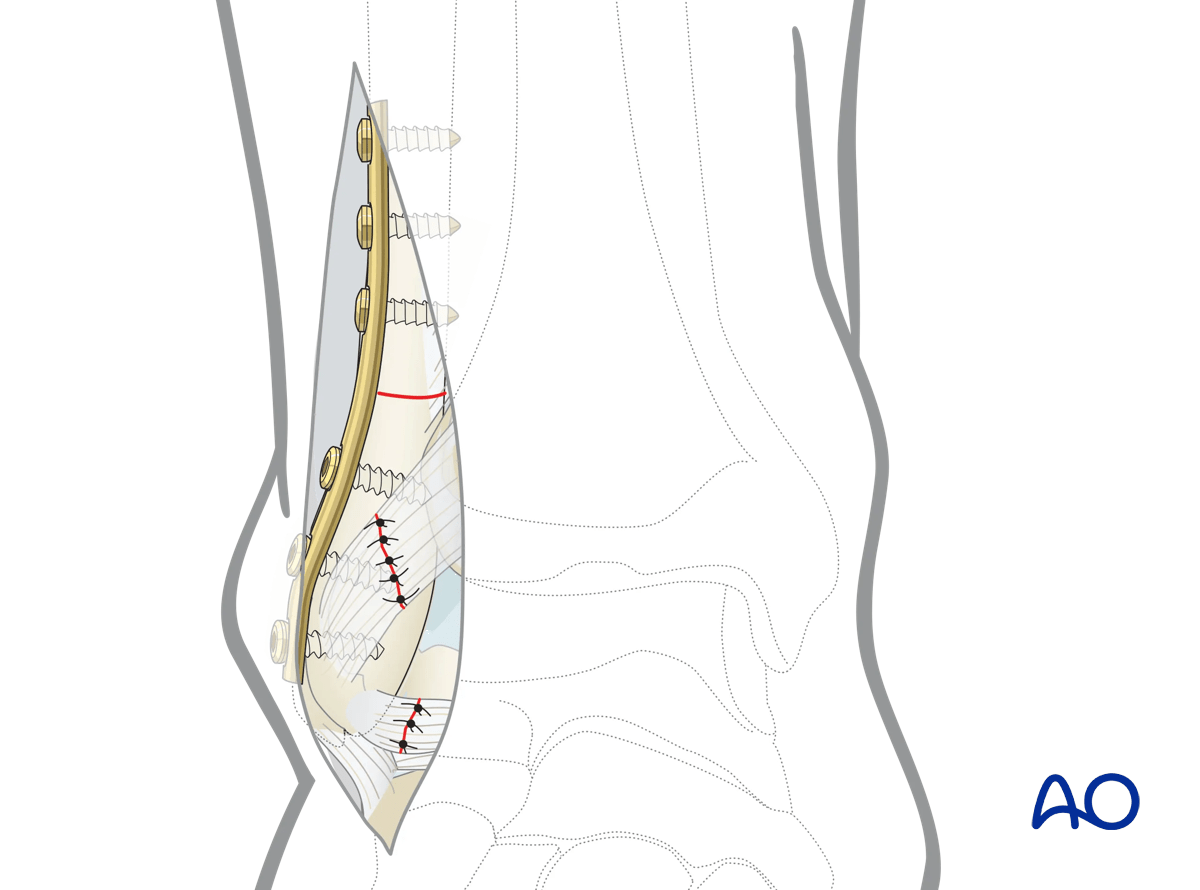
5. Repair
Once the internal fixation of the talus is finished, reduce the fibula anatomically. Stabilize the osteotomy with a carefully contoured plate in compression mode.
Alternatively, a longitudinal screw or fibular nail may be used for reconstruction of the osteotomy.
Primary repair of the anterior distal tibiofibular ligament can be attempted. If successful, the repair will restore the stability of the ankle. Suture anchors may be required to provide a sturdier ligamentous repair.
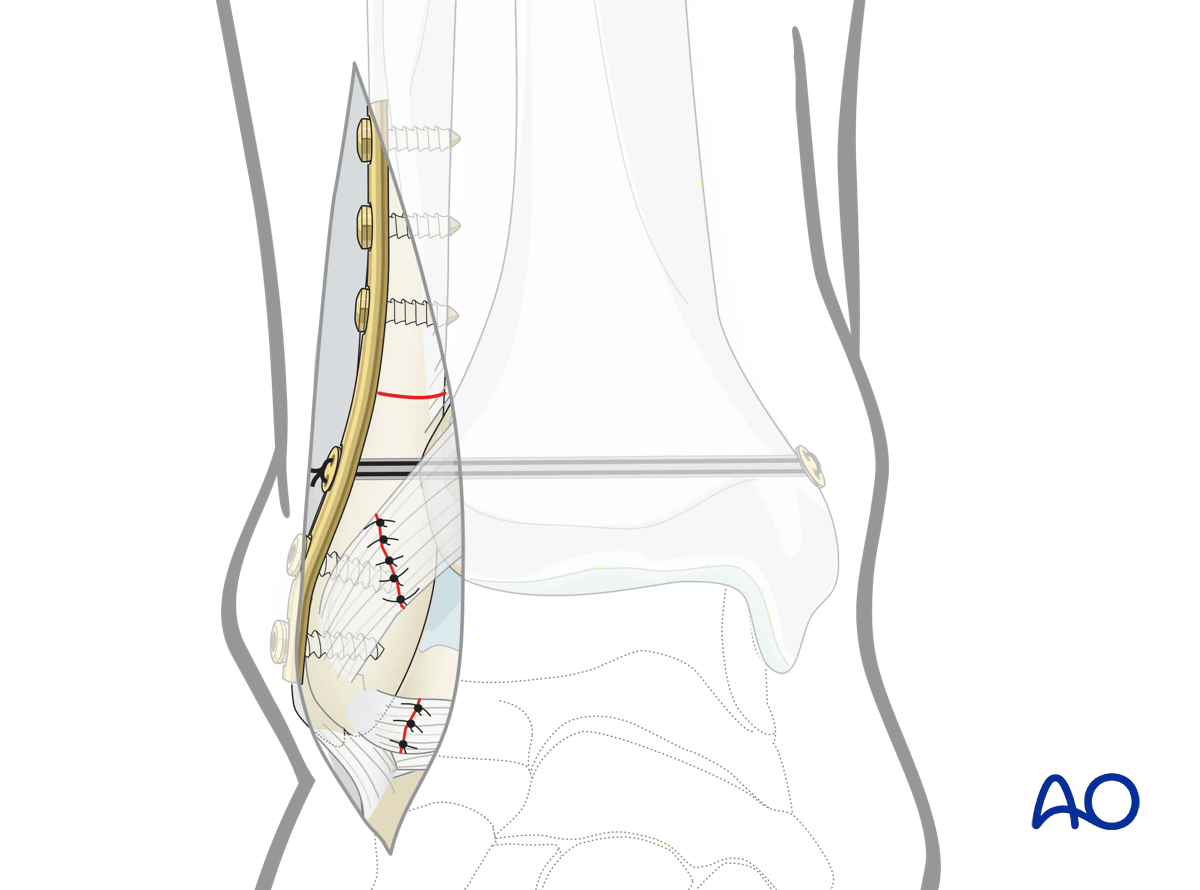
Additionally, syndesmotic stabilization may be required either with a suture and button (tightrope) or a screw.
6. Wound closure
This approach is closed in layers with deep sutures and skin sutures.