Anteromedial approach to the talus
1. Introduction
The anteromedial approach is usually employed in combination with the anterolateral approach to obtain an anatomic reduction of displaced and comminuted fractures.
This anteromedial approach allows for direct visualization of medial fracture reduction and for the insertion of a medially based fixation construct.
If a medial malleolar osteotomy is planned, the incision needs to be more inferior proximally.
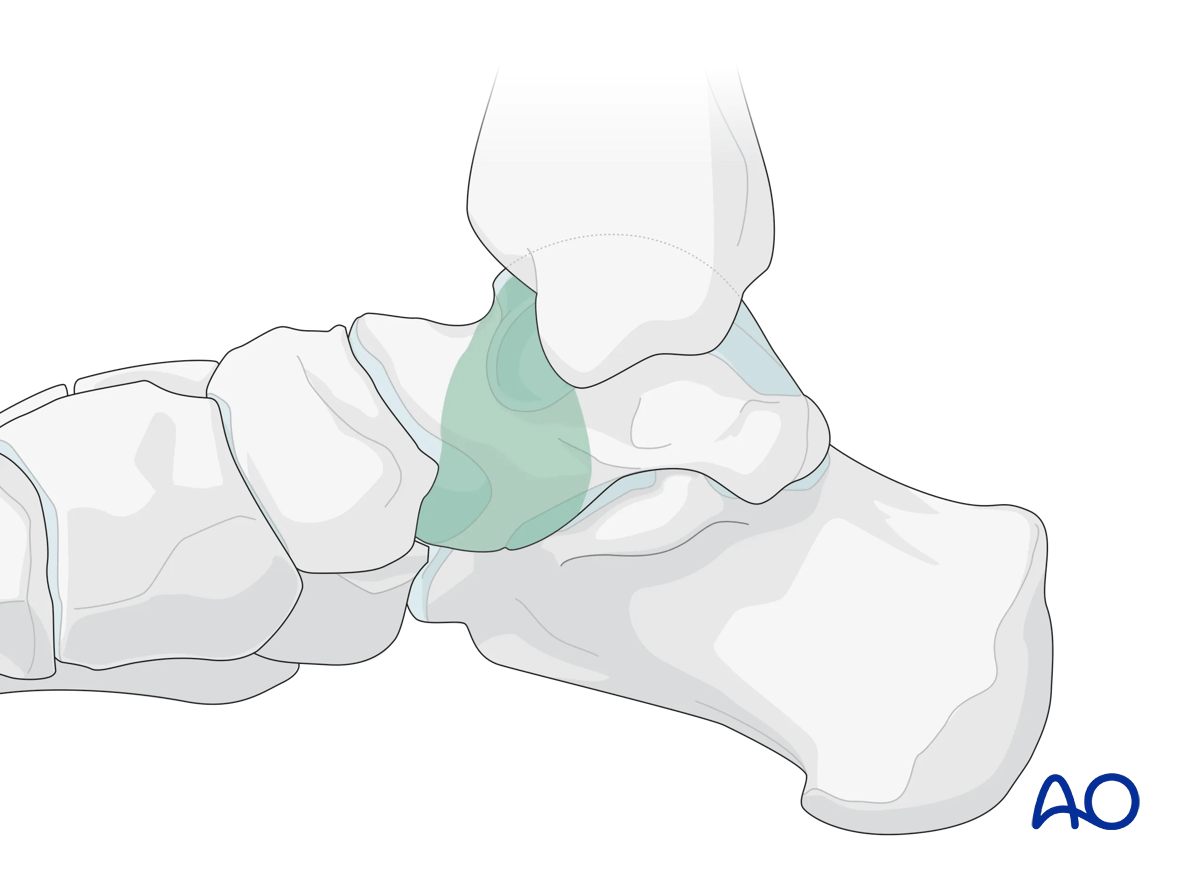
This illustration shows the areas of the talus that are visualized through this surgical approach.
2. Anatomy
Blood supply to the talus
Note: Fracture dislocations can easily compromise the blood supply to the body of the talus and lead to avascular necrosis.
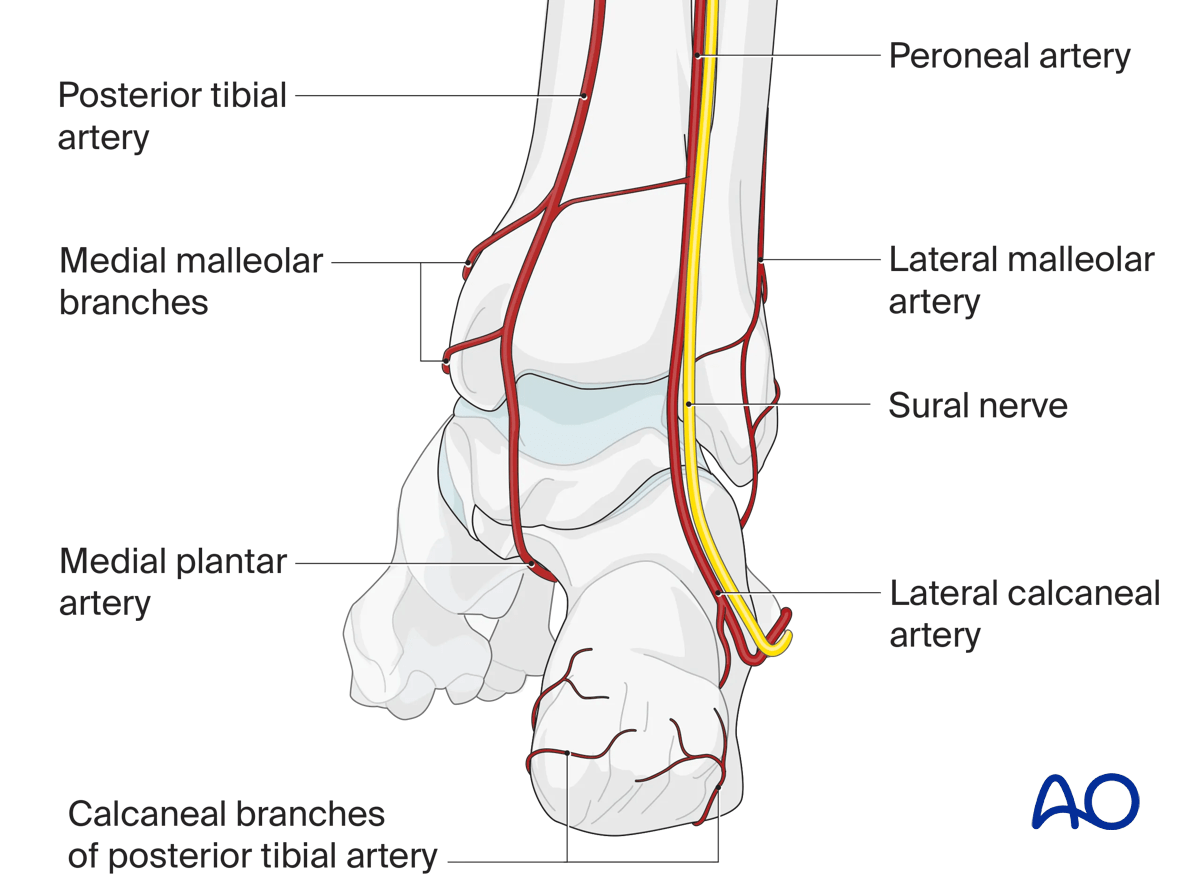
Anterior view with main arteries
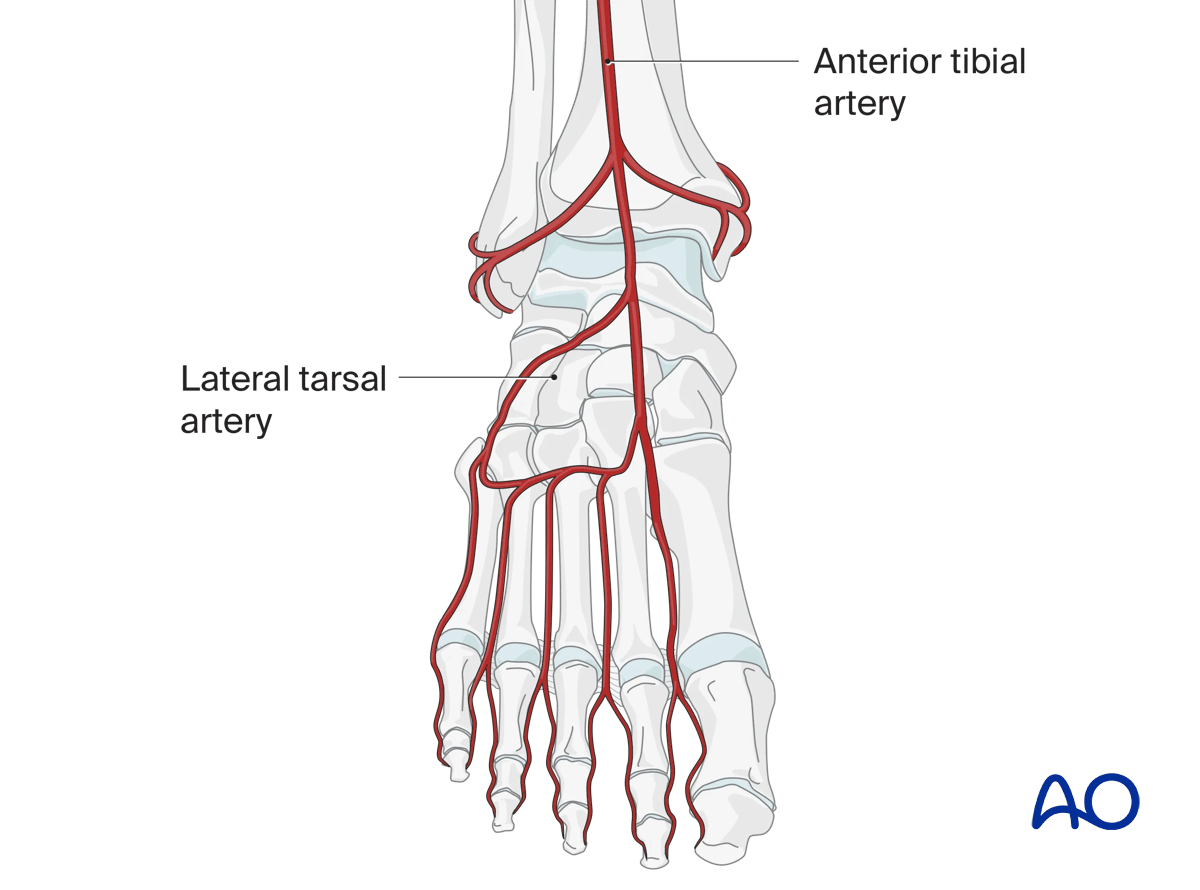
The talar neck receives arterial branches from the medial and lateral side (anterior and posterior tibial artery). The body of the talus is supplied almost exclusively from its posteromedial aspect.
The deltoid branches are important to supply blood to the medial talar neck and talar body. Branches from the dorsalis pedis supply the talar head and most of the dorsal talar neck.
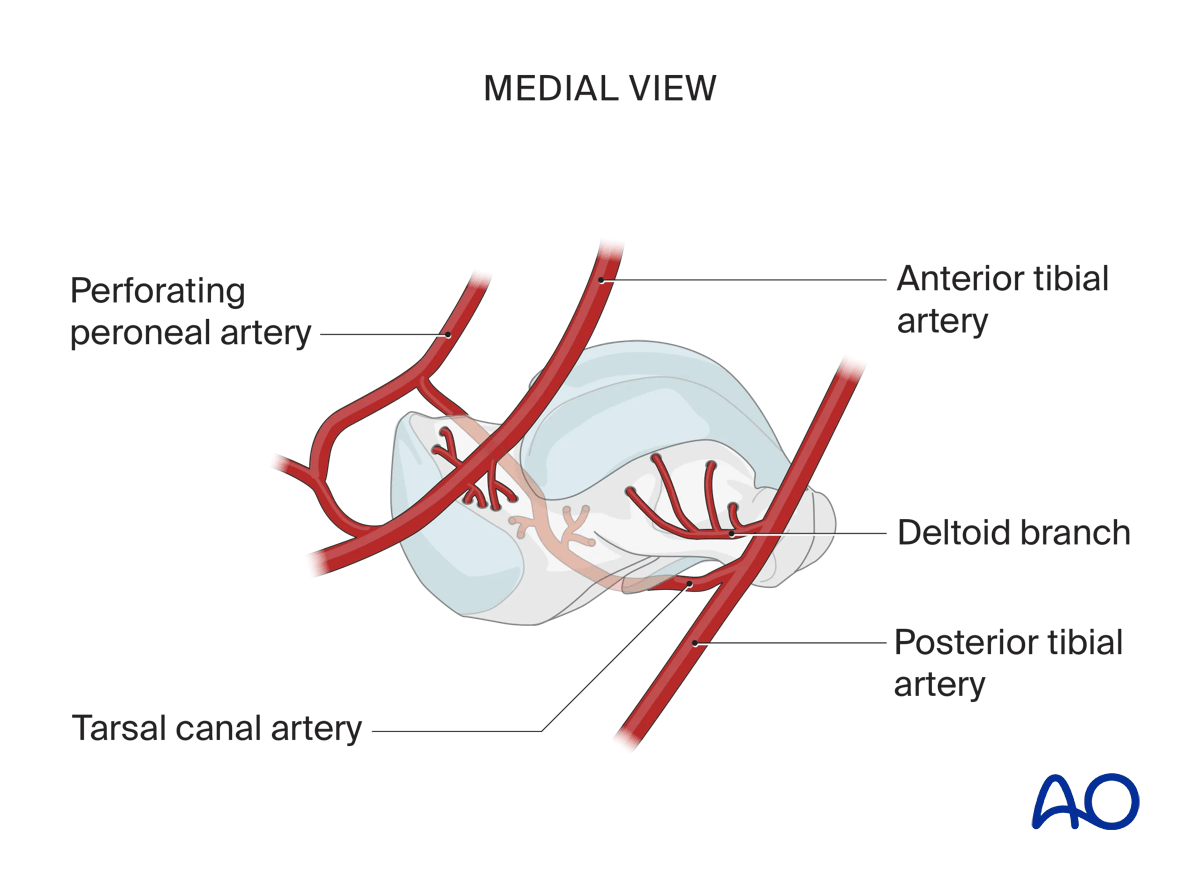
The artery of the tarsal canal coming from branches off the posterior tibial artery supplies most of the talar body.
The peroneal artery has the least contribution laterally.
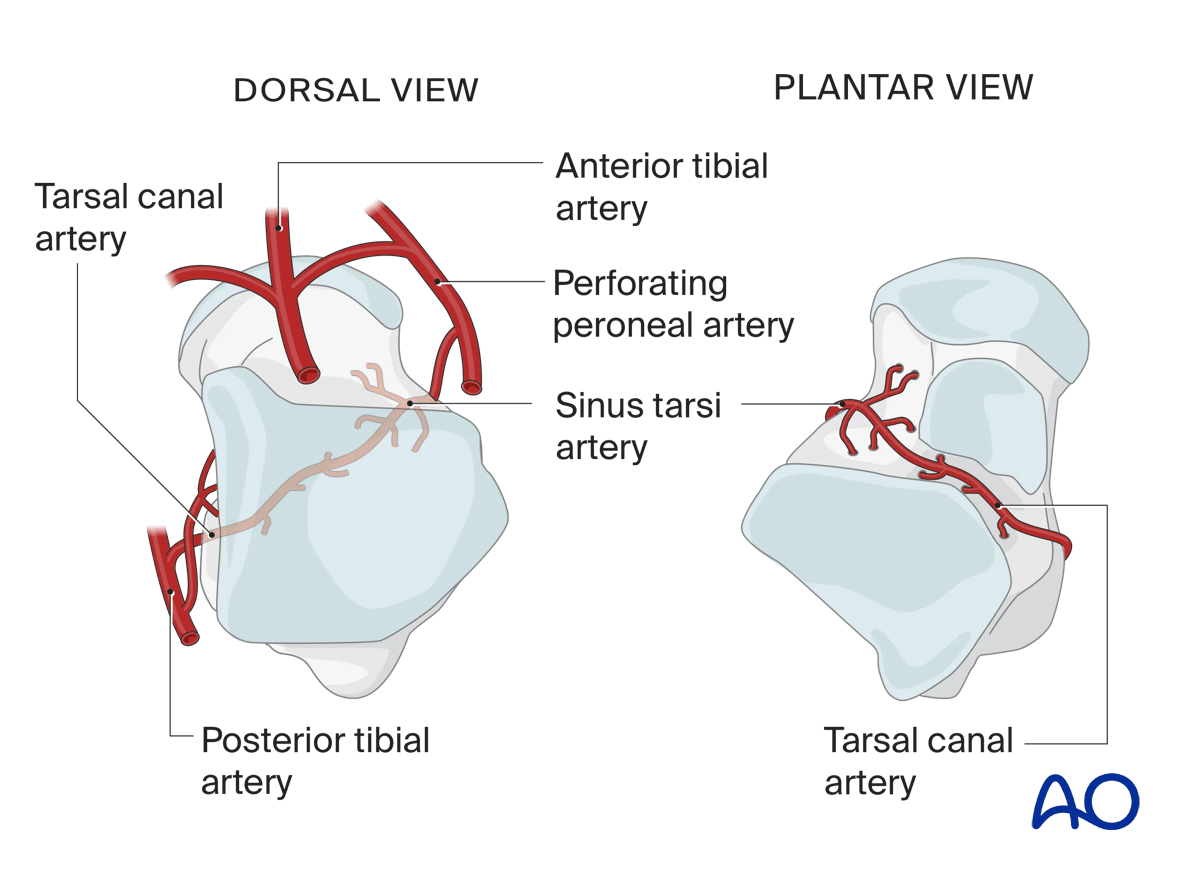
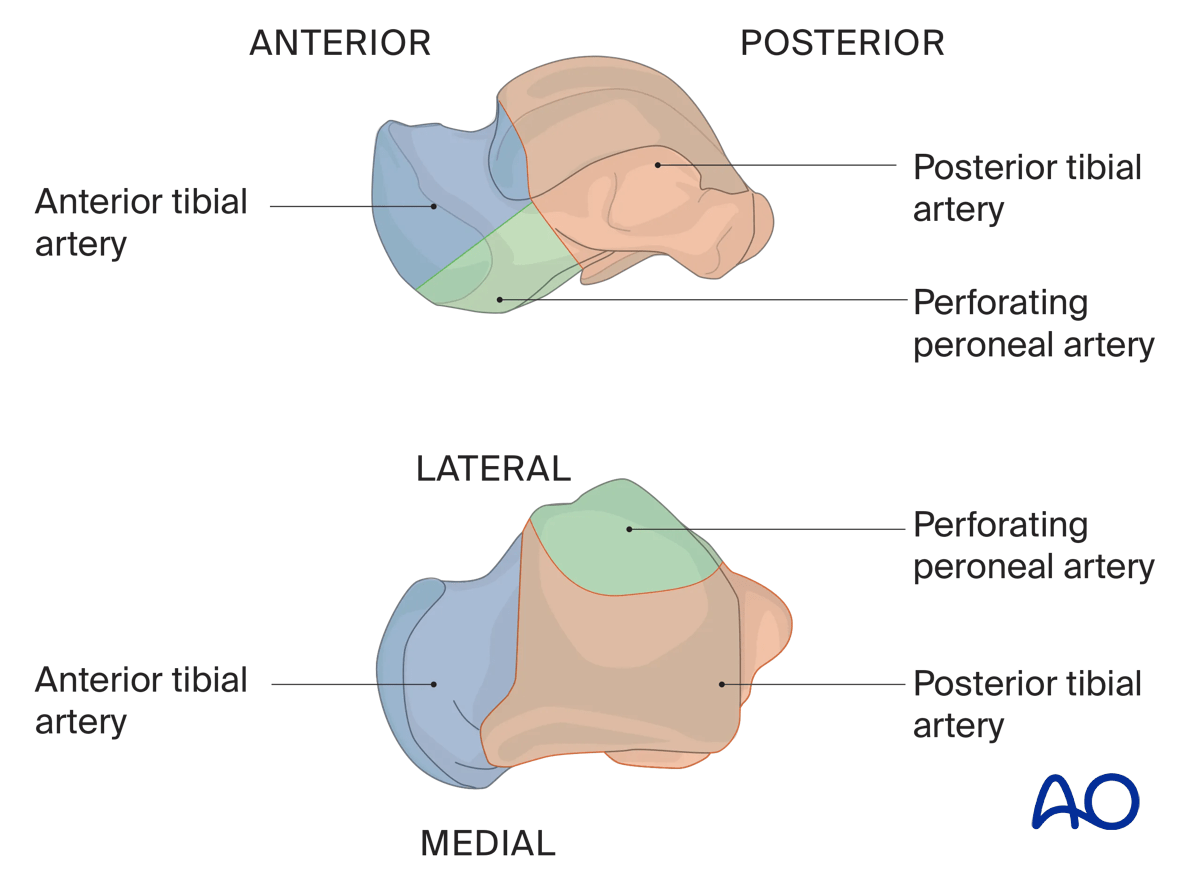
Illustration showing the contribution of arterial blood supply to the talus:
- Anterior tibial artery (blue)
- Posterior tibial artery (orange) including the deltoid branch
- Perforating peroneal artery (green)
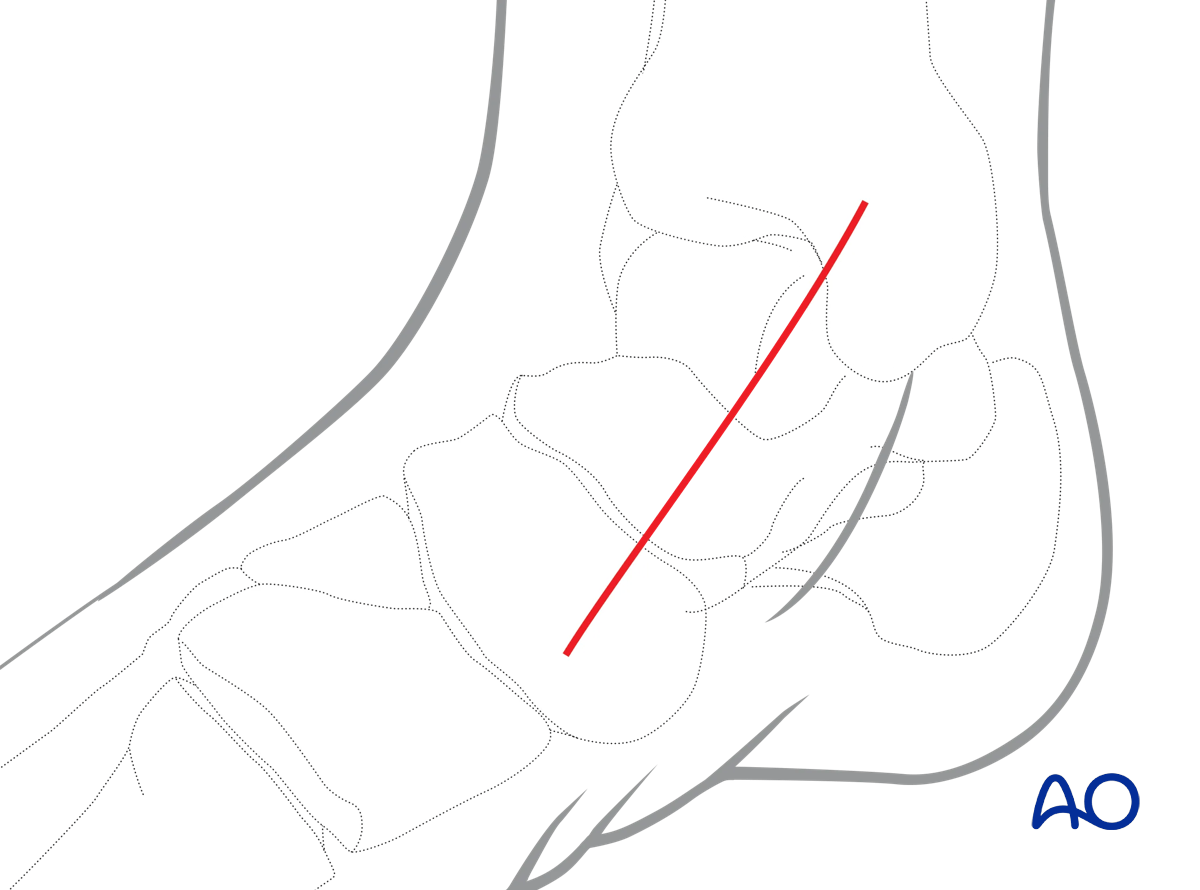
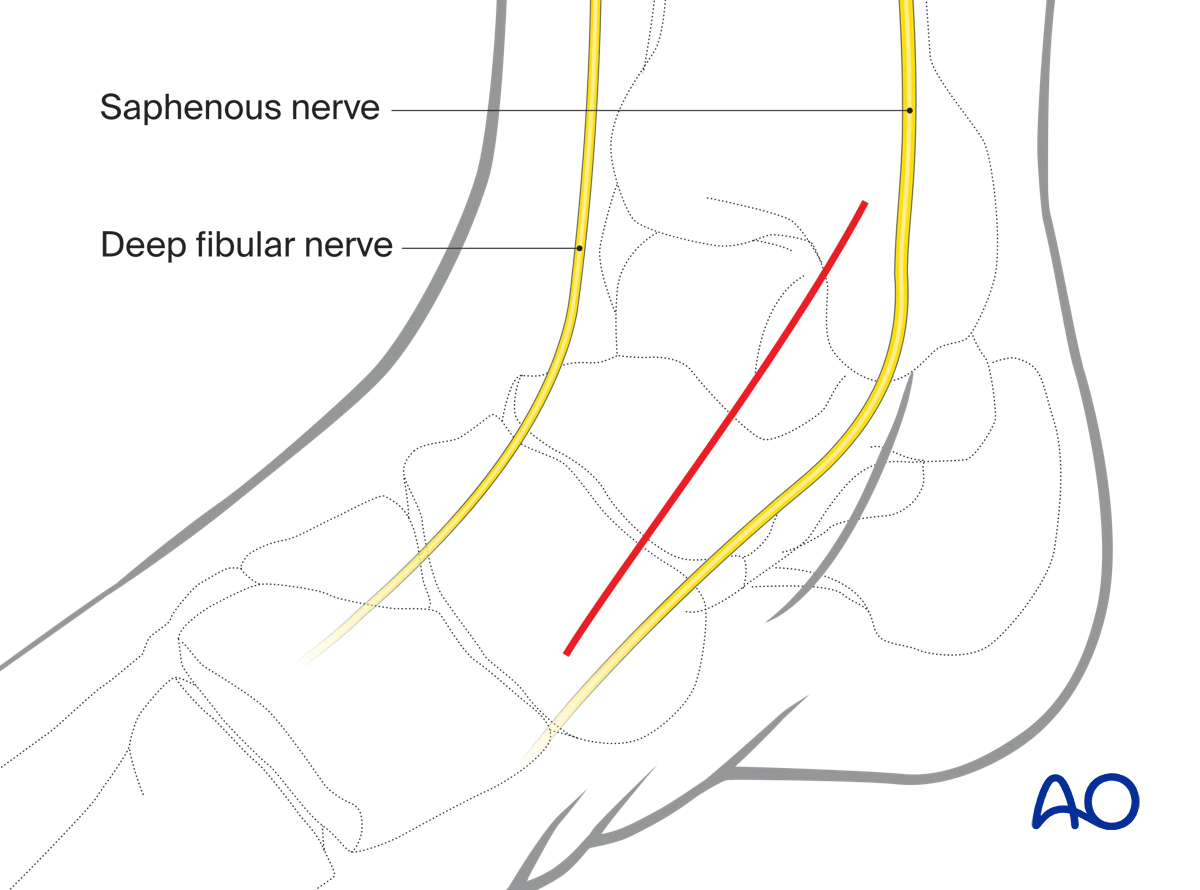
3. Skin incision
Perform an incision starting at the medial malleolus and extending distally to the navicular.
For more complex fractures, particularly those requiring a medial malleolar osteotomy, the incision may be extended proximally.
The precise position and length of the incision depend on the fracture configuration and patient anatomy.
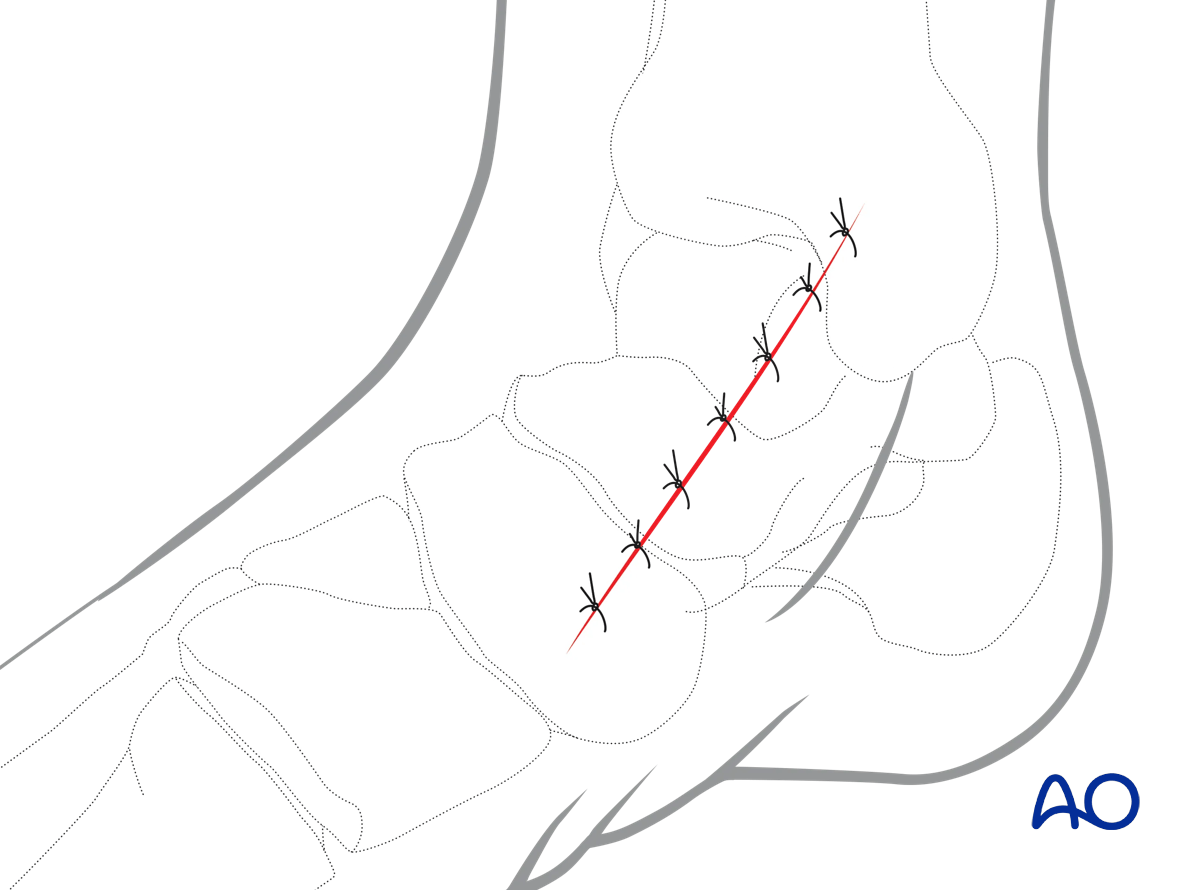
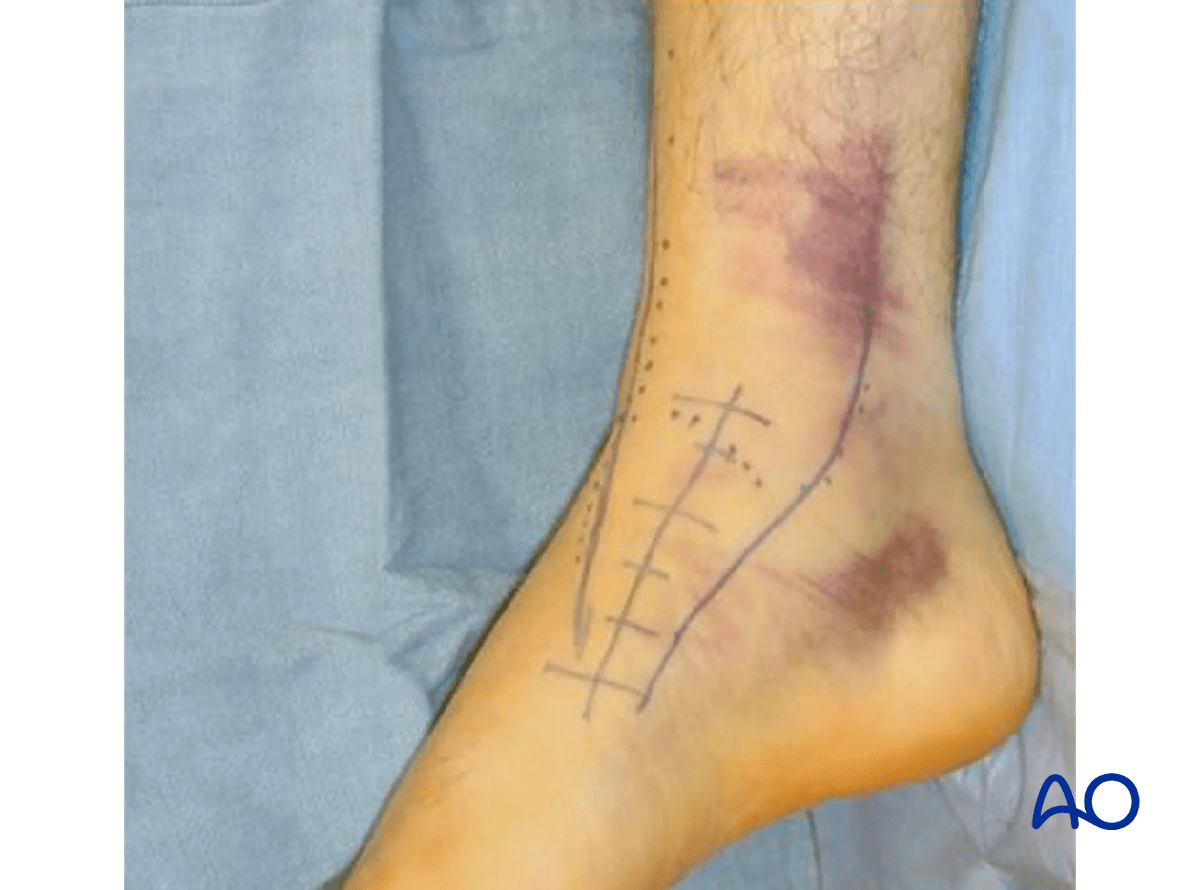
Preoperative marking of the incision
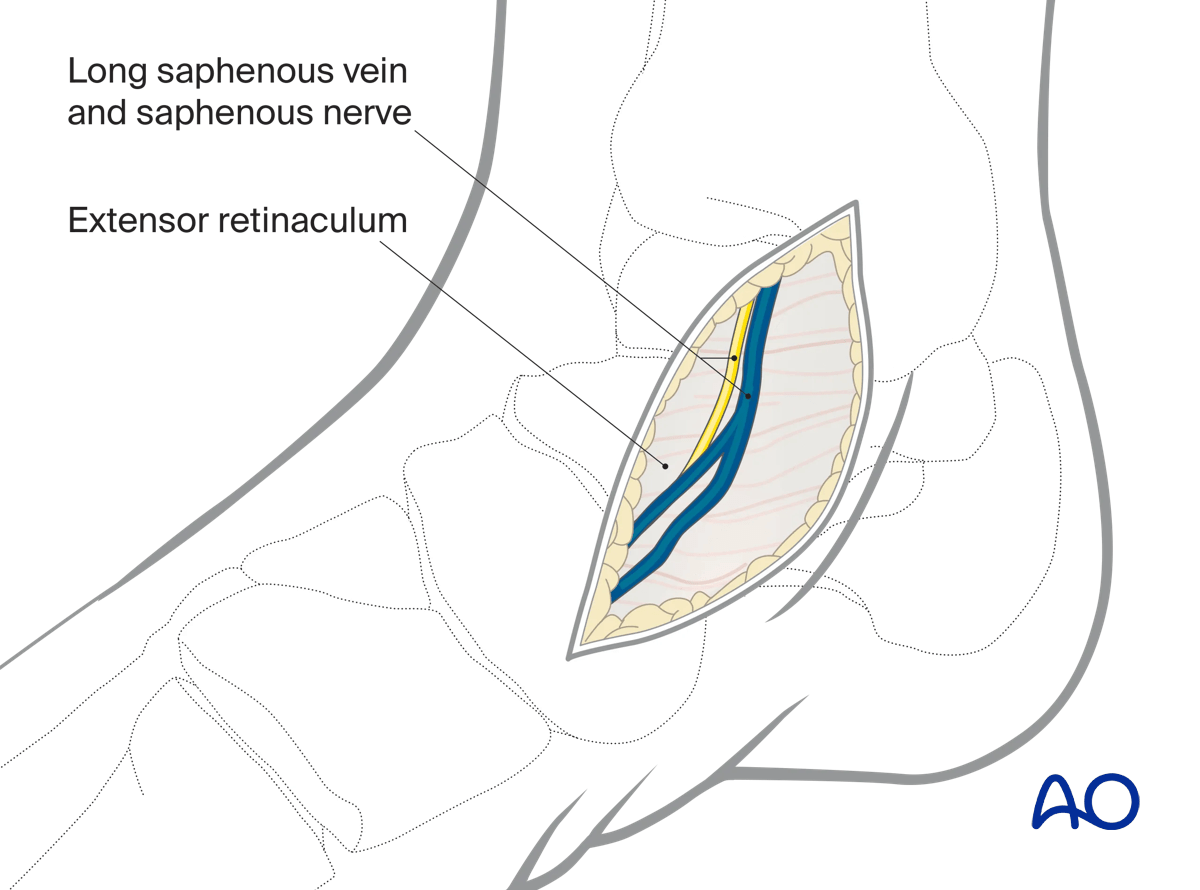
After incising through skin, identify the long saphenous vein and nerve. The vein and its branches may need to be ligated or coagulated.
Be careful not to damage the deltoid arterial branches which arise posteromedially and supply the medial two thirds of the talar body.
Minimize periosteal stripping of the talus to avoid damage to the blood supply.
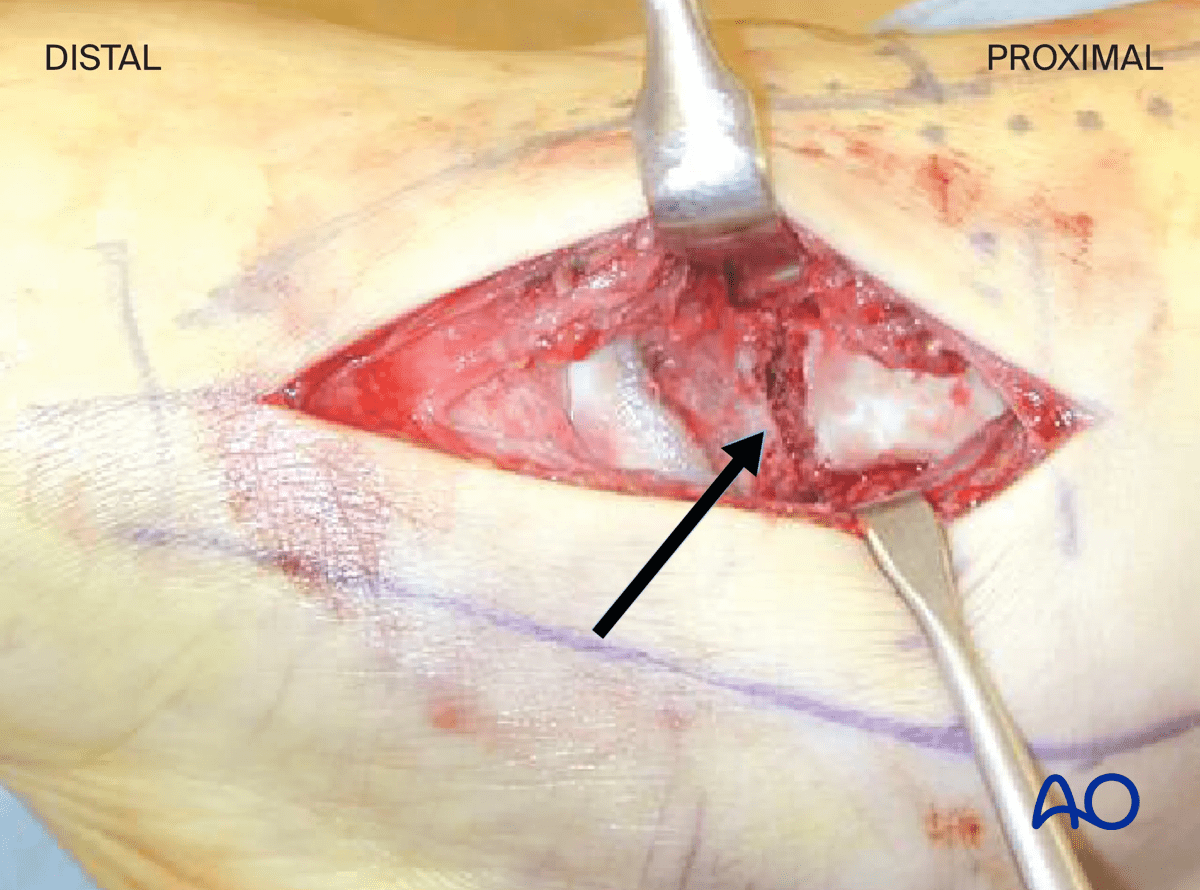
4. Exposure of the anteromedial talar neck
Once skin is incised and the medial talus identified, evacuate the fracture hematoma to expose the underlying inferomedial aspect of the neck and the fracture.
The arrow points to a simple fracture of the talar neck.
5. Wound closure
This approach is closed in two layers.