Anterolateral approach to the talus
1. Introduction
Many talar neck fractures are commonly exposed with two combined approaches, anterolateral and anteromedial.
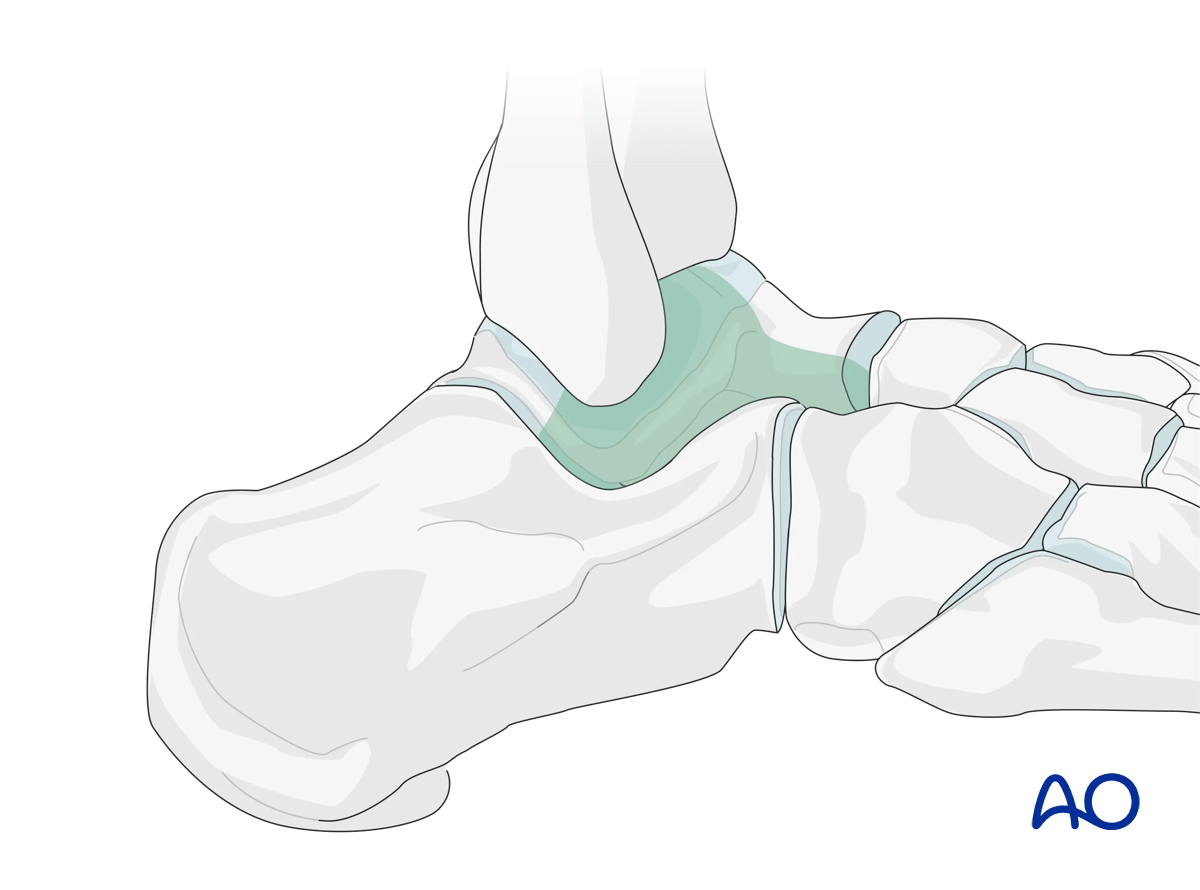
The anterolateral approach allows for direct visualization of lateral talar neck, fracture reduction, debridement of the subtalar joint, identification and treatment of lateral process fractures, and for the insertion of laterally based fixation.
This illustration shows the areas of the talus that are visualized through this surgical approach.
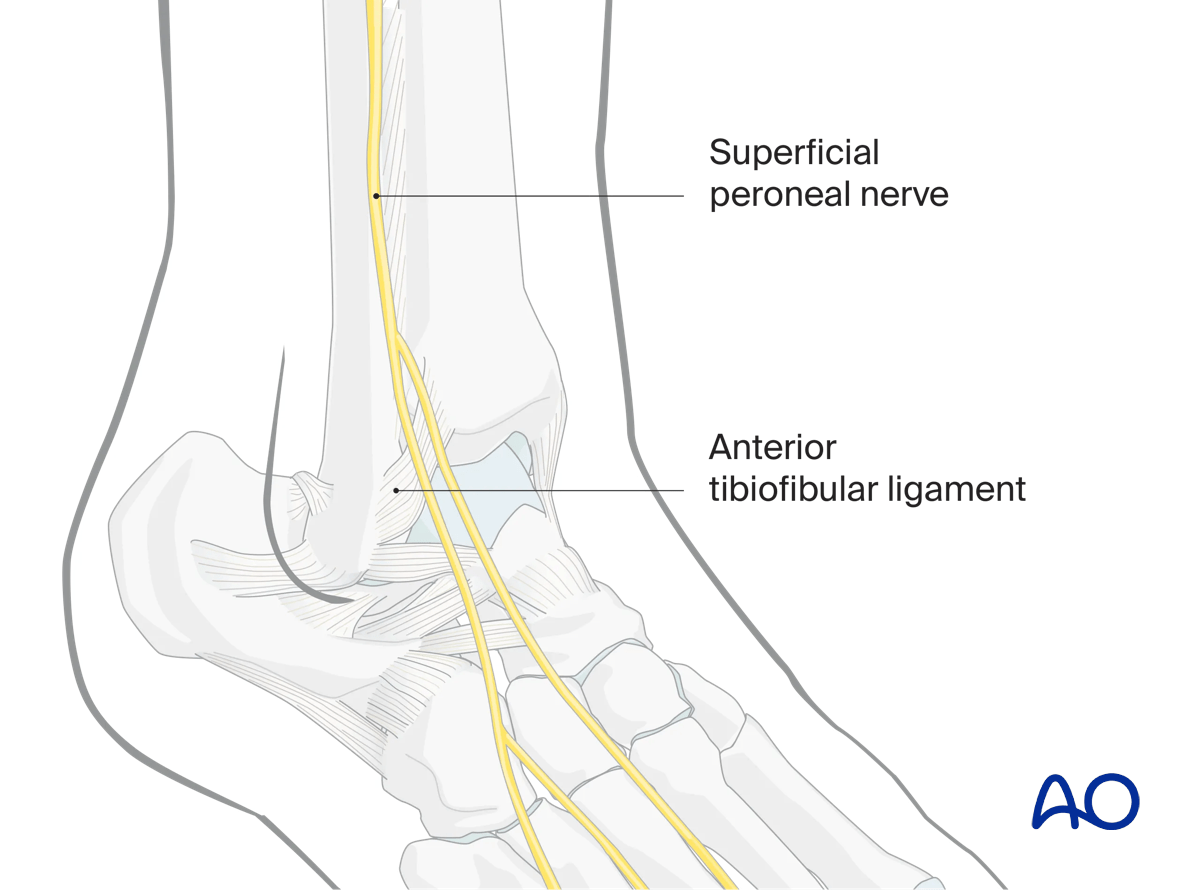
2. Anatomy
Immediately anterior to the fibula lies the superficial branch of the peroneal nerve. Its location is variable and must be protected with this approach.
The anterior distal tibiofibular and talofibular ligaments may be incised to improve exposure, but caution should be given due to their structural importance.
The peroneal blood supply is a posterior structure and is not endangered with this approach.
Blood supply to the talus
Note: Fracture dislocations can easily compromise the blood supply to the body of the talus and lead to avascular necrosis.
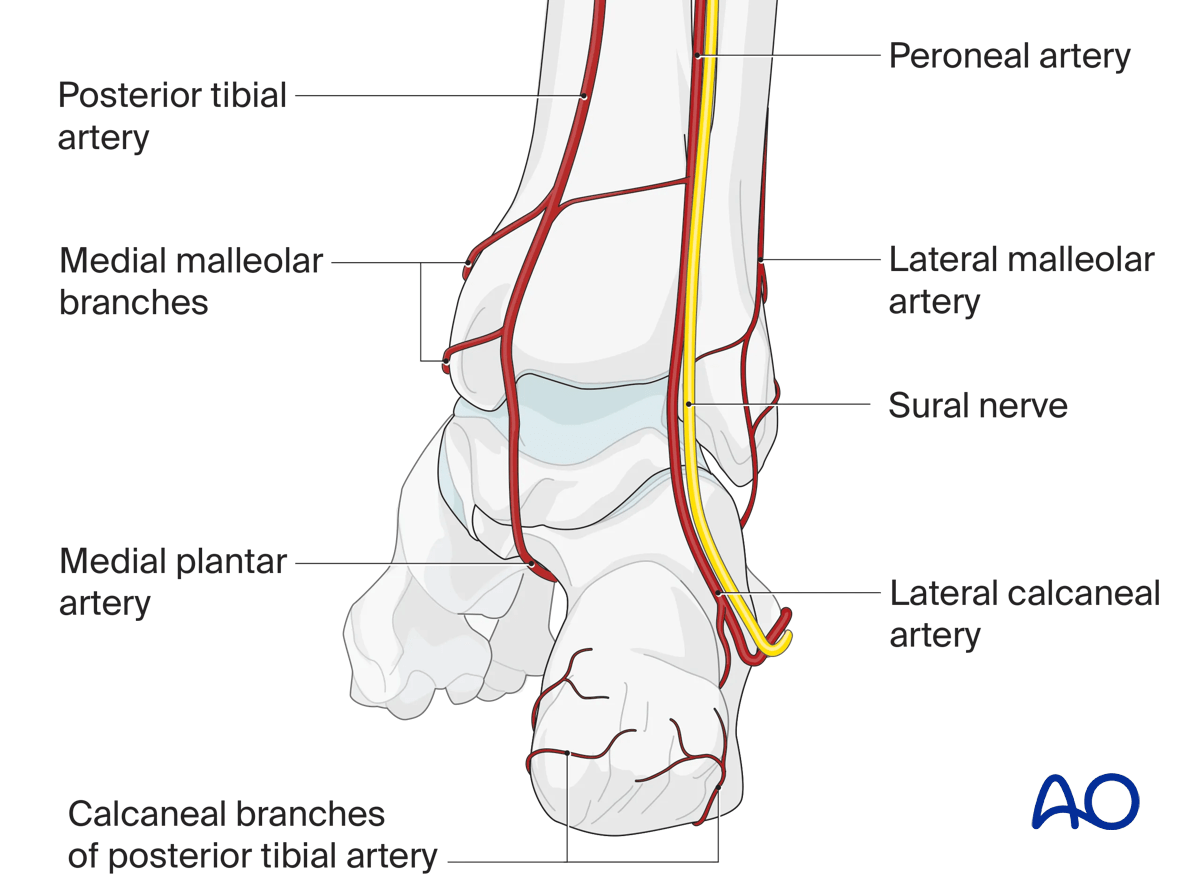
Anterior view with main arteries
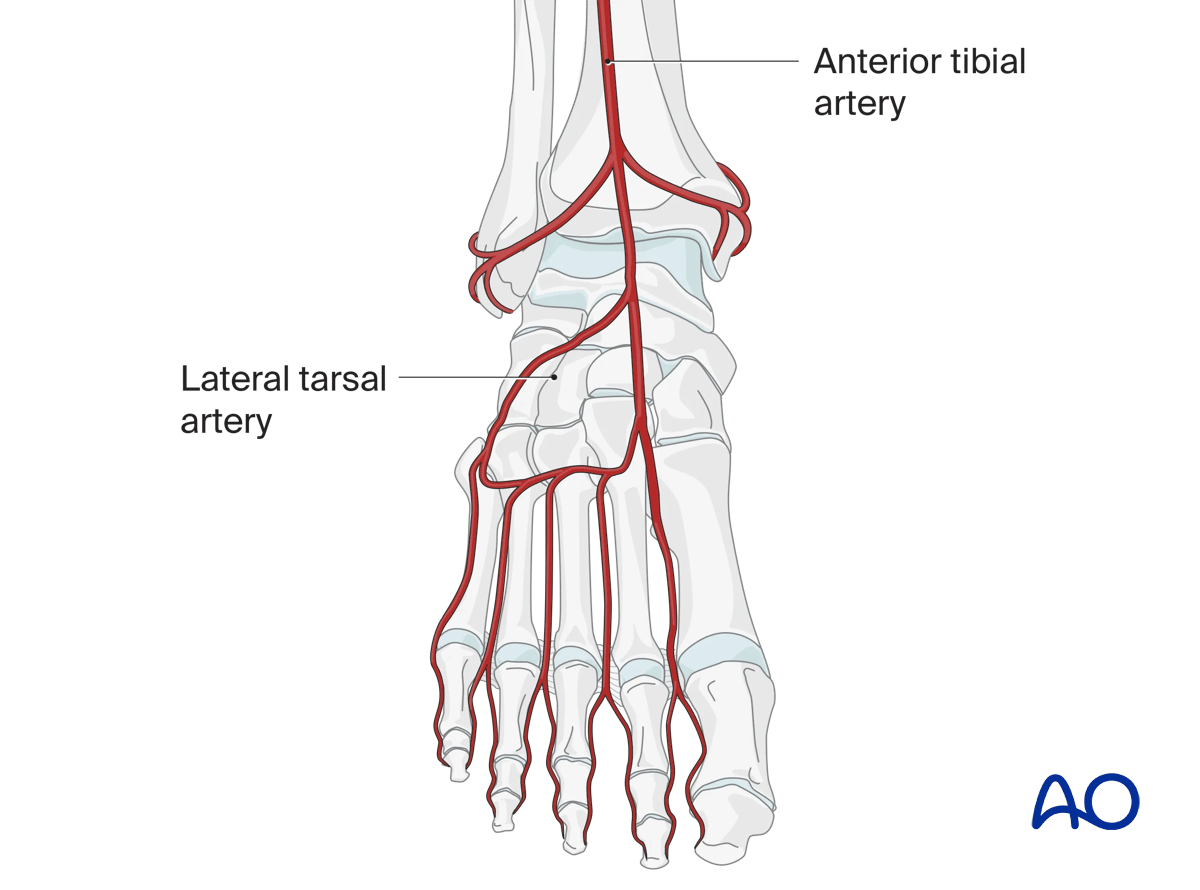
The talar neck receives arterial branches from the medial and lateral side (anterior and posterior tibial artery). The body of the talus is supplied almost exclusively from its posteromedial aspect.
The deltoid branches are important to supply blood to the medial talar neck and talar body. Branches from the dorsalis pedis supply the talar head and most of the dorsal talar neck.
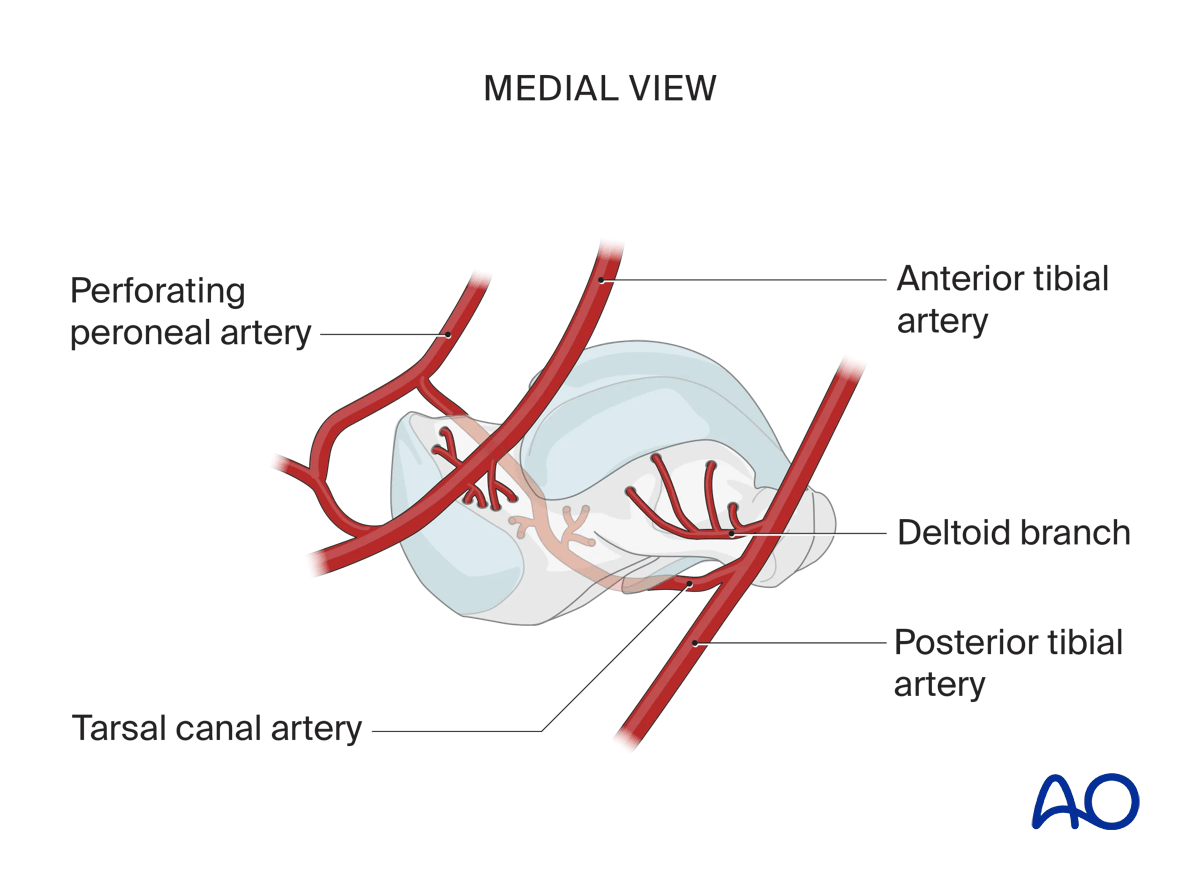
The artery of the tarsal canal coming from branches off the posterior tibial artery supplies most of the talar body.
The peroneal artery has the least contribution laterally.
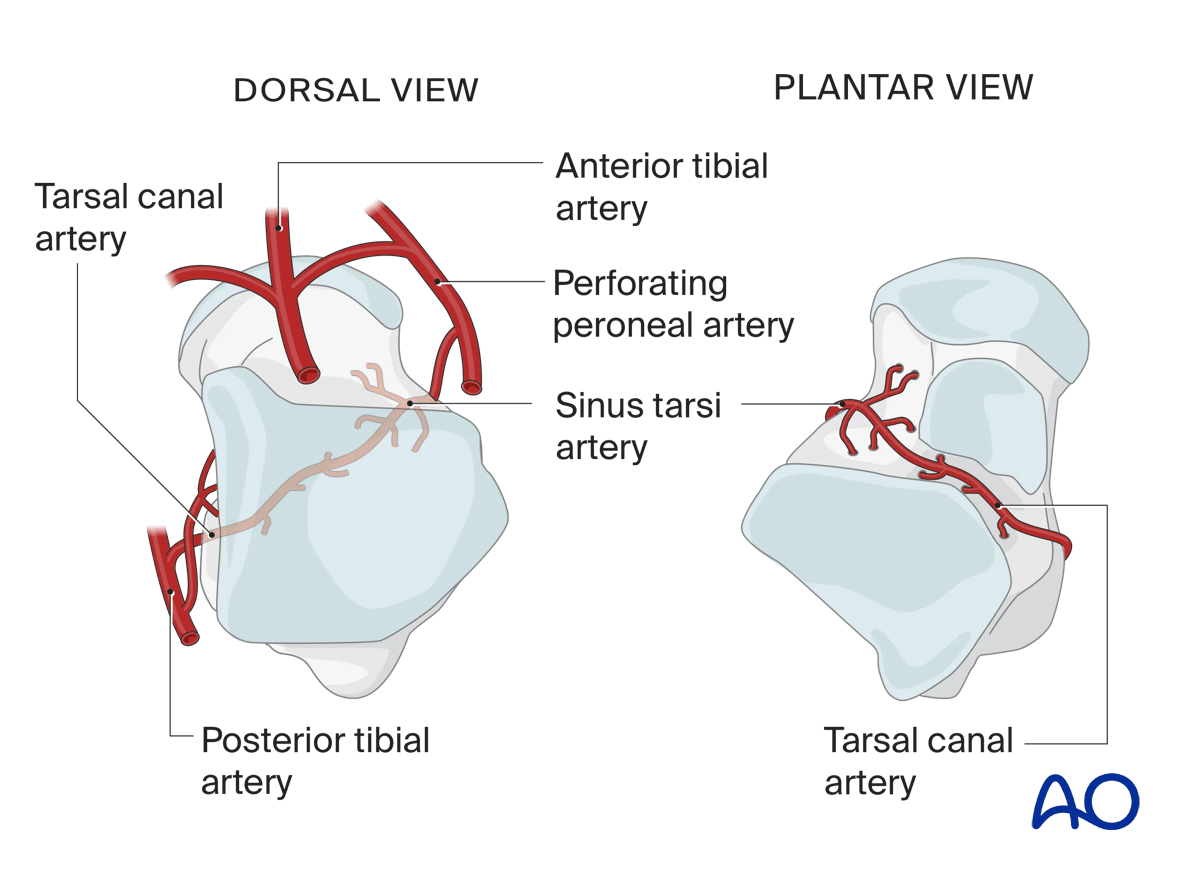
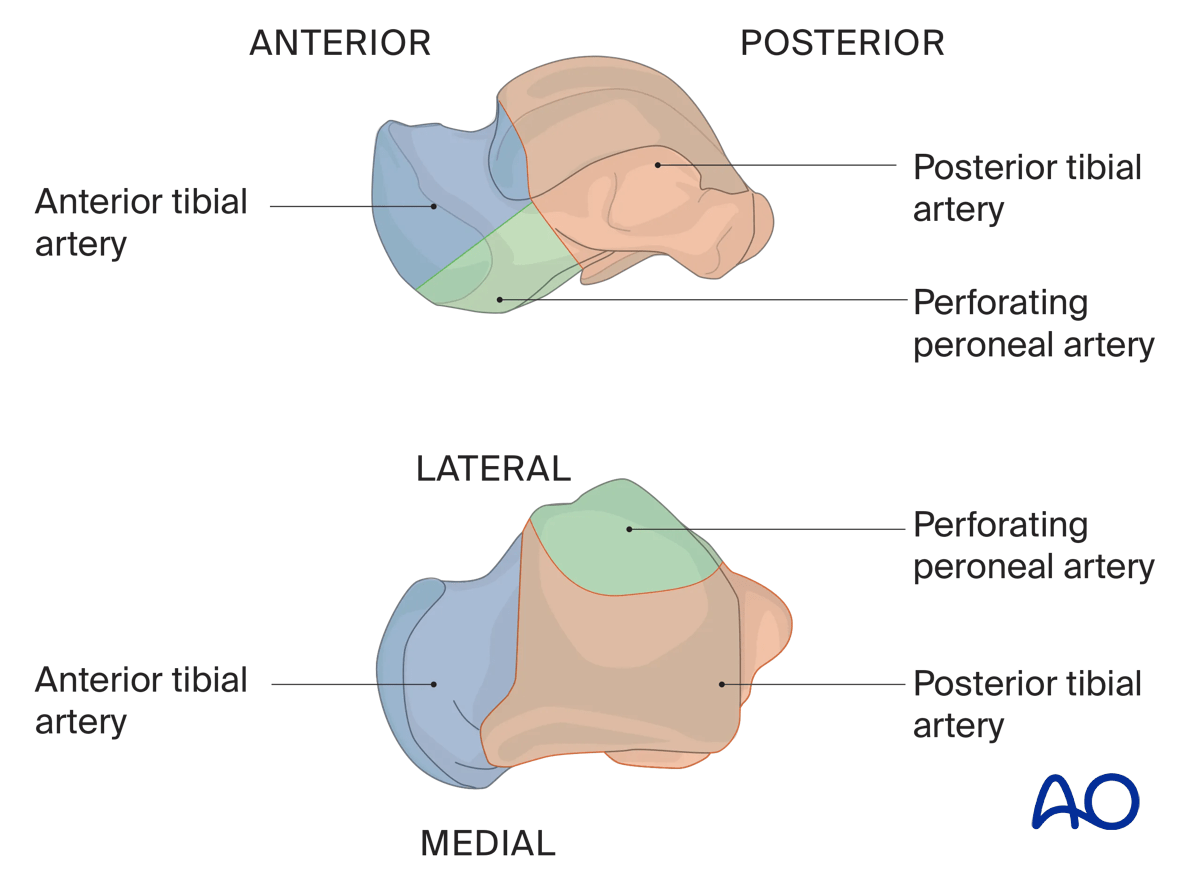
Illustration showing the contribution of arterial blood supply to the talus:
- Anterior tibial artery (blue)
- Posterior tibial artery (orange) including the deltoid branch
- Perforating peroneal artery (green)
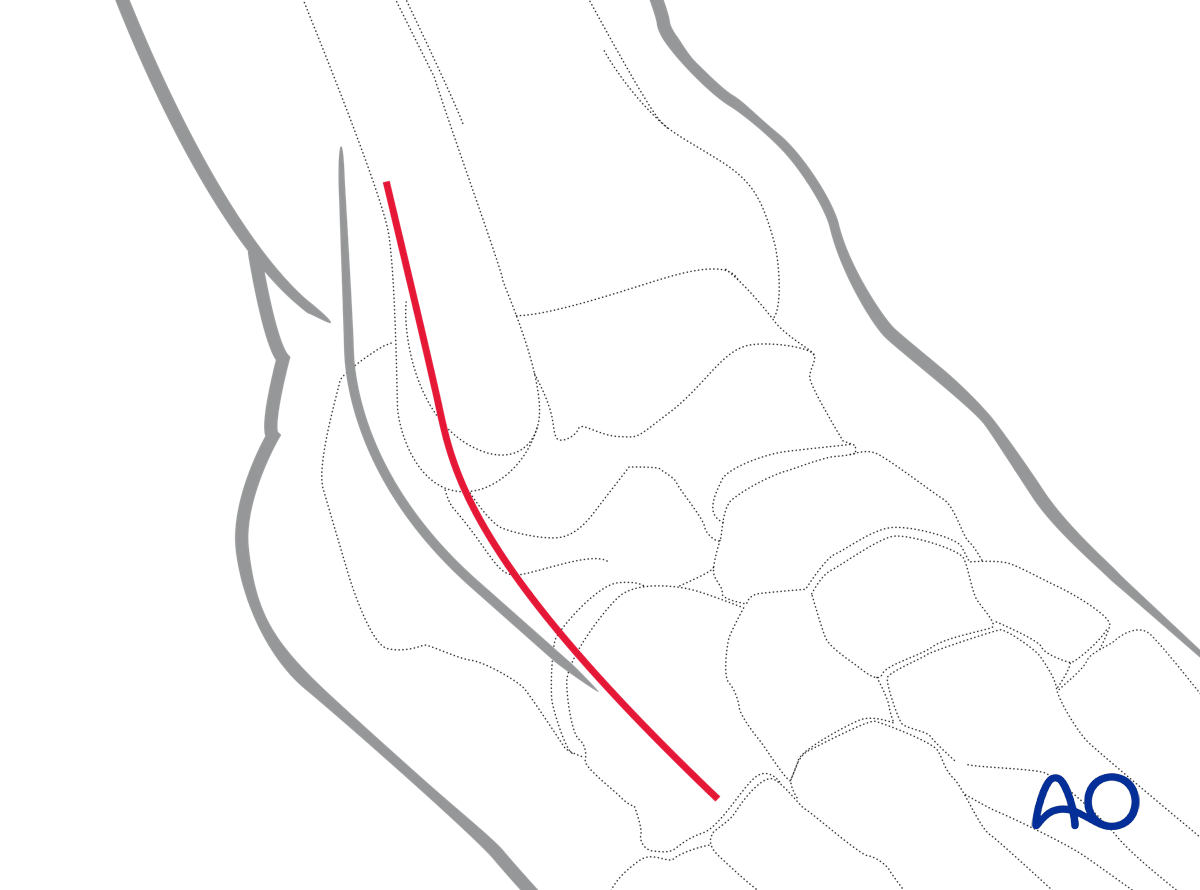
3. Incision
Skin incision
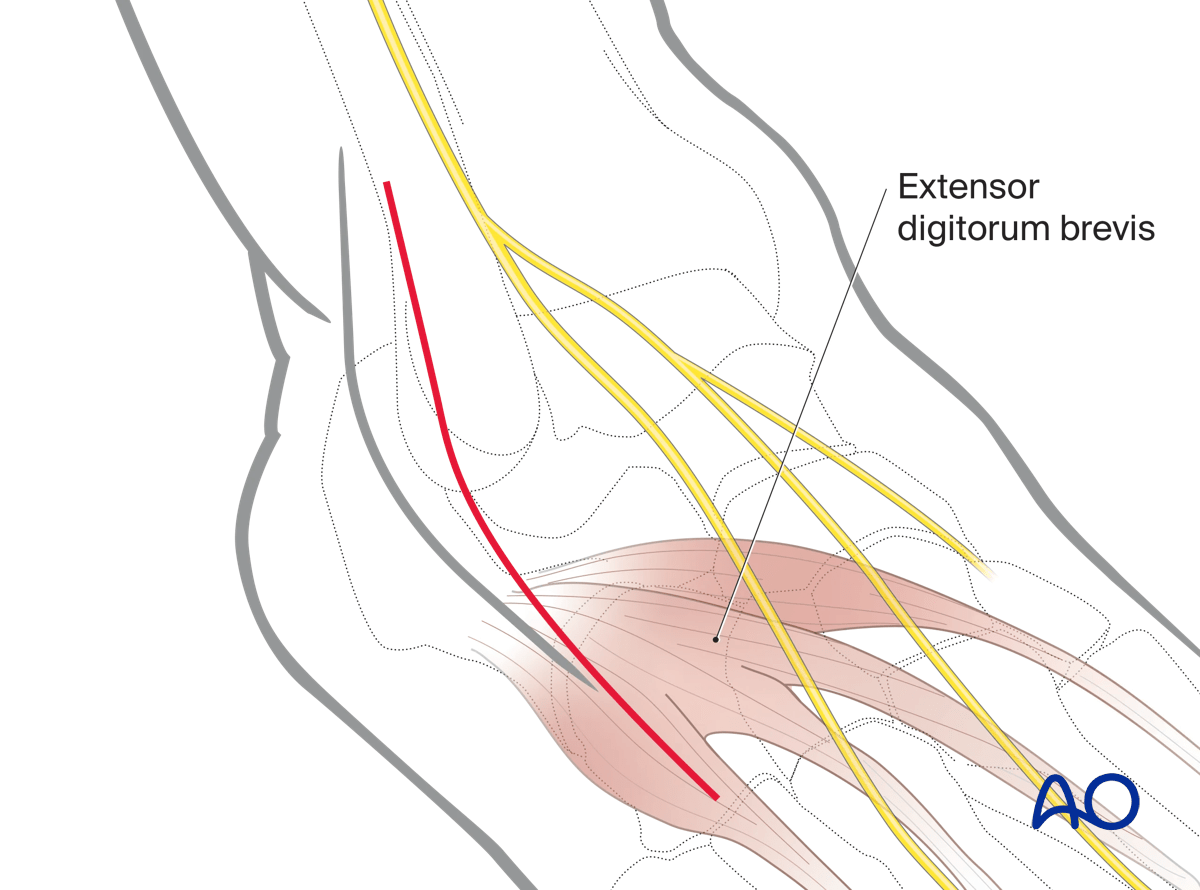
Around the ankle and hindfoot, full-thickness incisions without undermining are imperative. To avoid cutting the branches of the superficial peroneal nerve, the incision must be made longitudinally.
The incision is based along the axis of the 4th metatarsal. It extends from the distal end of the fibula to the base of the 4th metatarsal.
The precise position and length of the incision depend on the fracture configuration and patient anatomy.
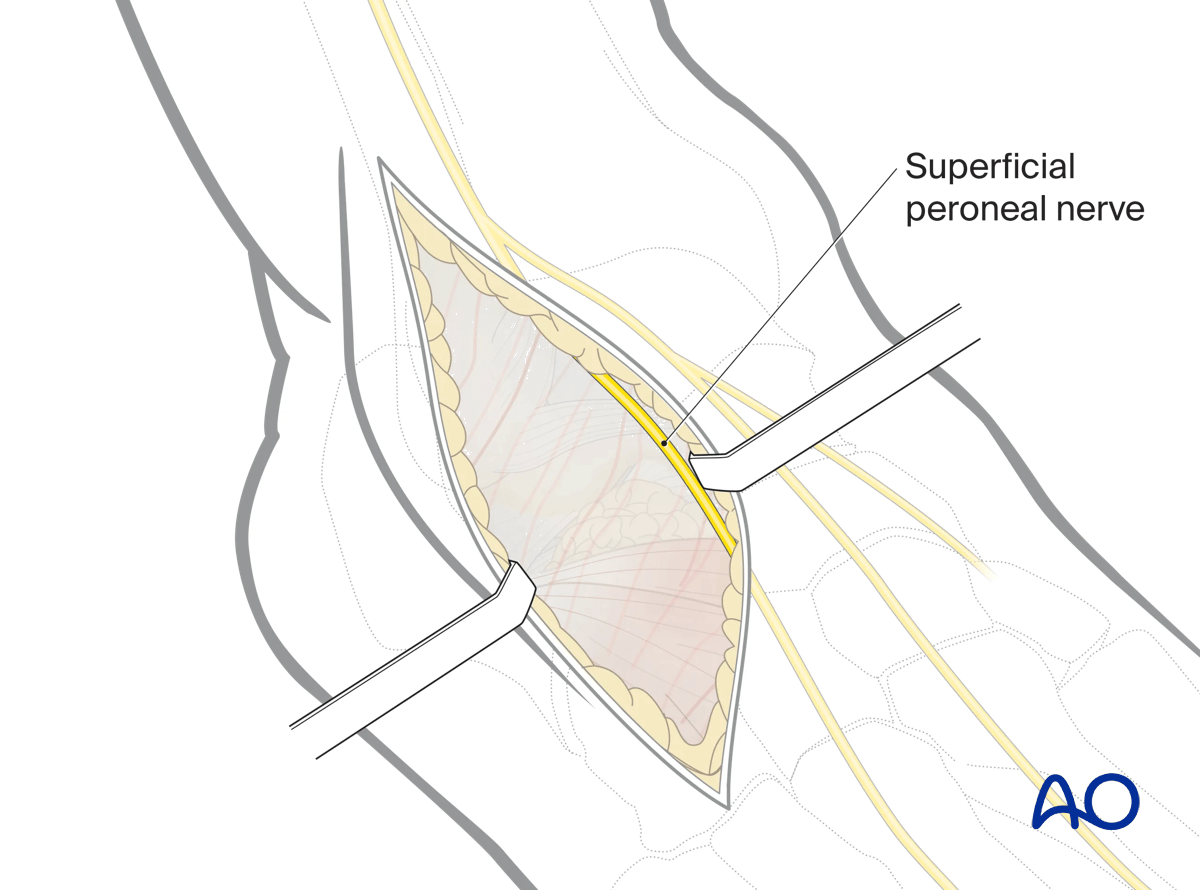
After the skin is incised, protect the superficial peroneal nerve either by identifying it or by avoiding it by the placement of the incision.
Depending on the precise position of the incision, the peroneal nerve is usually on the medial side of the incision.
Deep dissection
Divide the deep fascia and extensor retinaculum leading down to the extensor digitorum brevis.
This muscle is bulky but once it is released, …
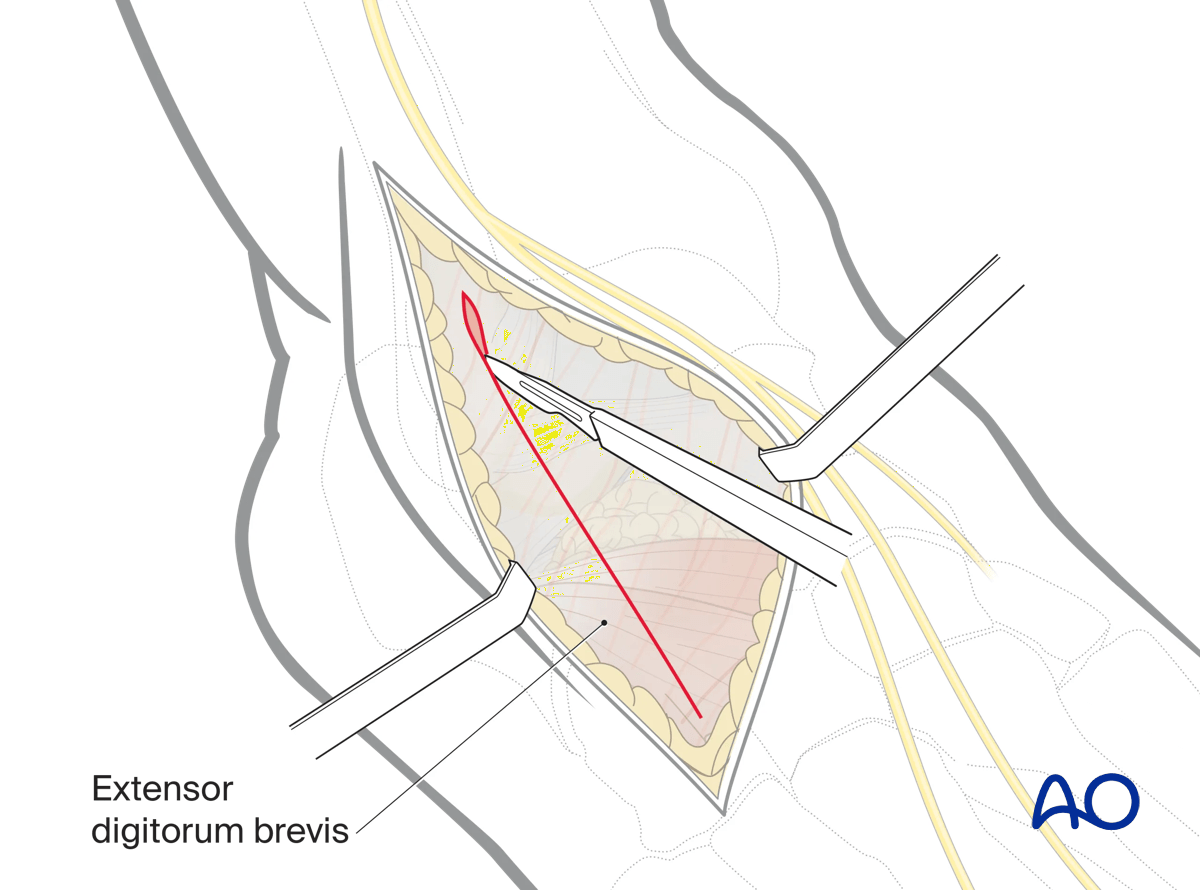
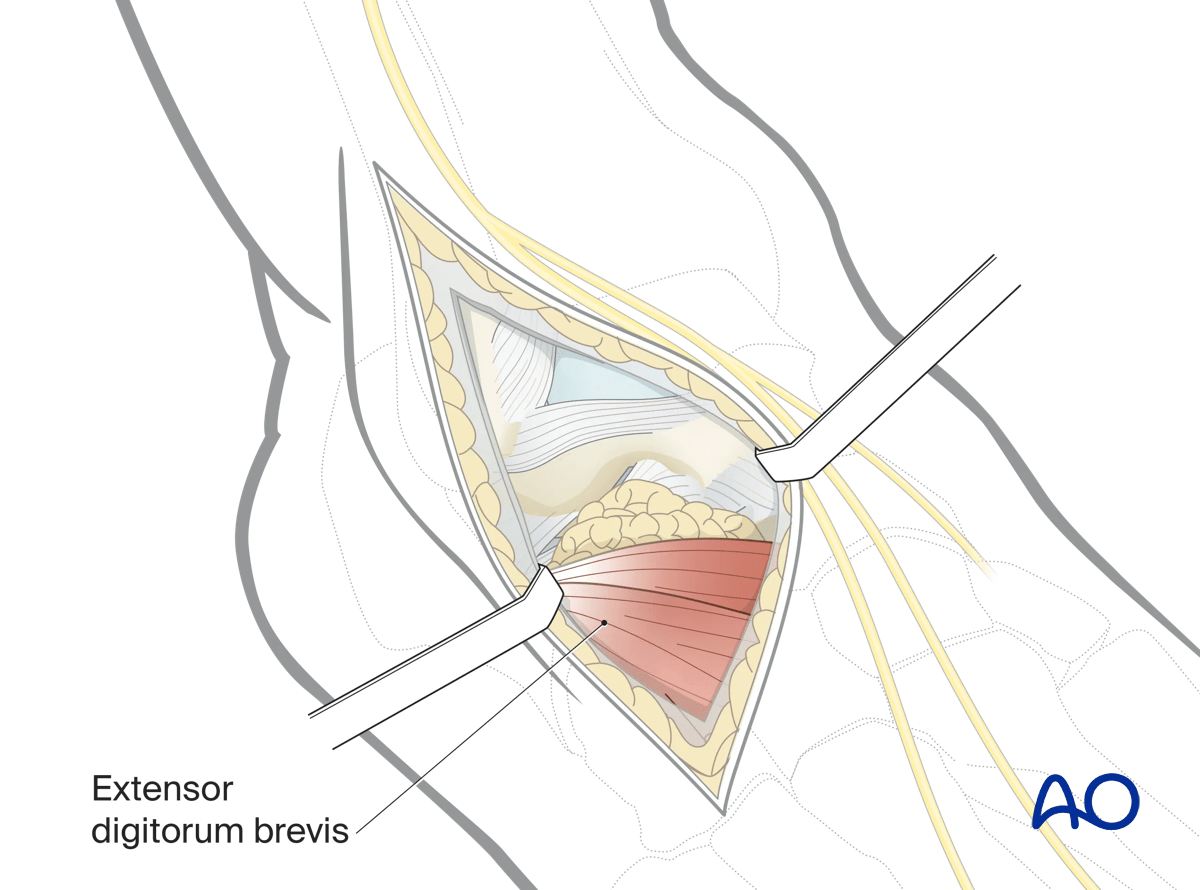
… one gains access to the lateral talus and subtalar joint.
4. Exposure of the anterolateral talar neck
Once the extensor digitorum brevis is retracted, the lateral aspect of the talar neck is exposed.
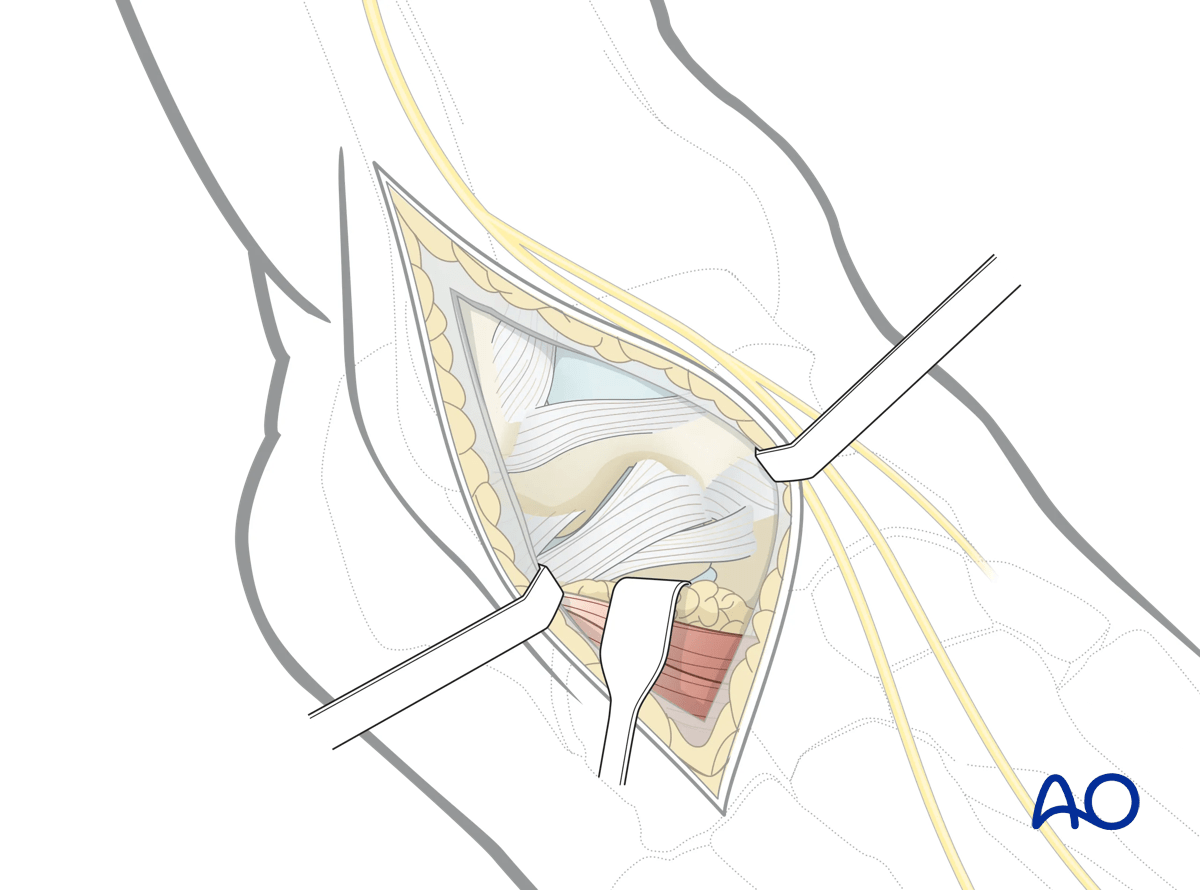
Debridement of subtalar joint
Debride and wash out the subtalar joint prior to reduction and stabilization.
5. Wound closure
This approach is closed in layers restoring all the anatomic structures.














