Straight lateral approach to the proximal tibia
1. Introduction
The straight lateral approach is preferred for exposure and fixation of fractures involving the proximal fibula and proximal tibiofibular joint. It allows safe visualization and manipulation of the common peroneal nerve.
2. Skin incision
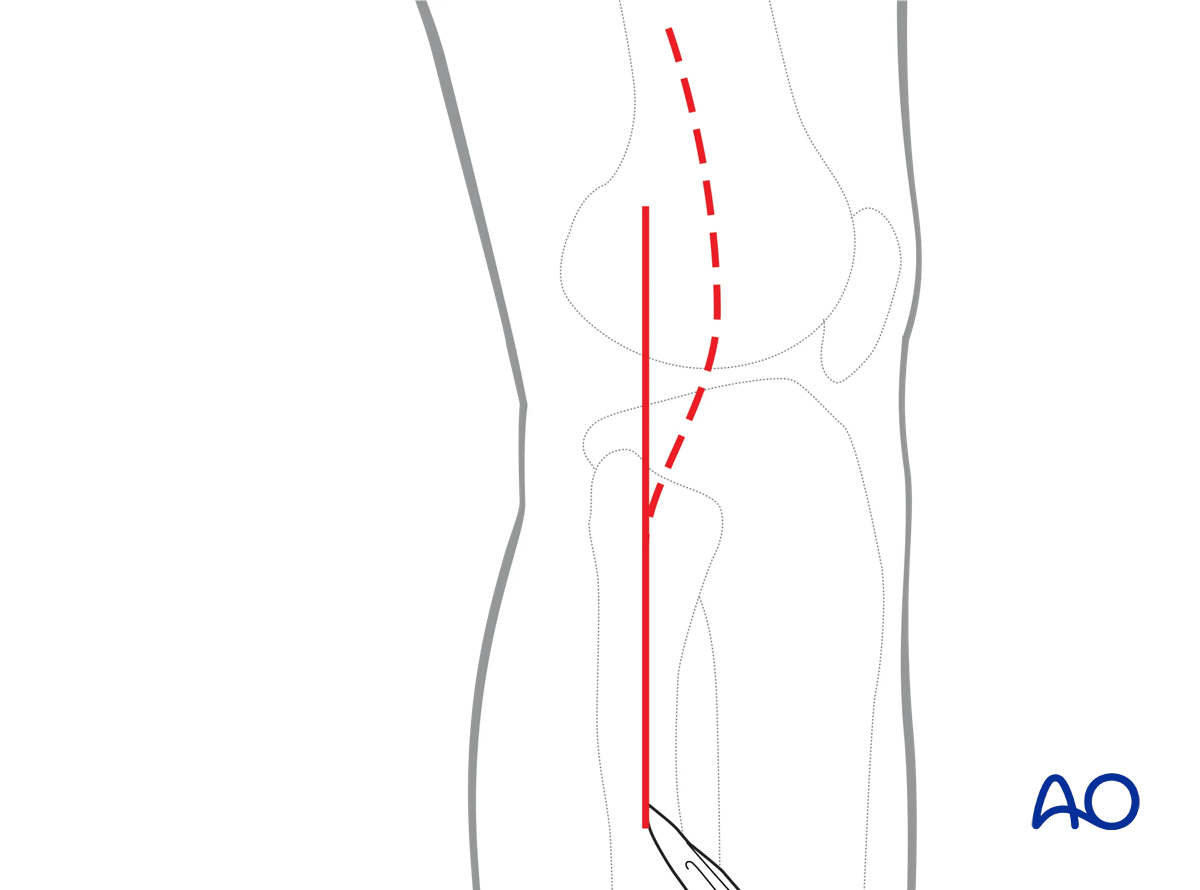
A longitudinal skin incision can be made directly over the head of the fibula. If access to the lateral tibial plateau is required, the skin incision may be placed more anteriorly or combined with a curvilinear anterolateral approach.
3. Opening the fascia
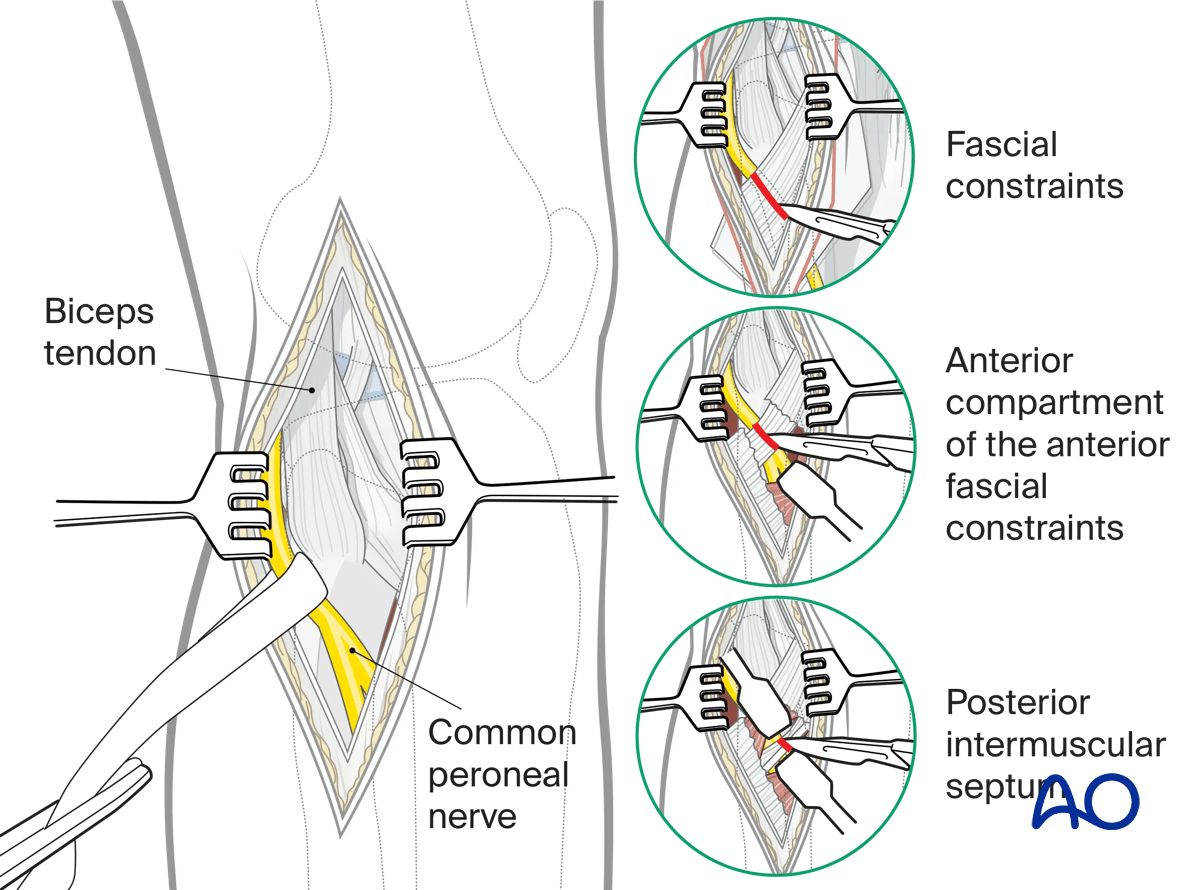
The skin and subcutaneous tissue are incised. The deep fascia should be identified and carefully opened with Metzenbaum scissors. The primary focus should now be identification of the common peroneal nerve. This can be localized immediately posterior to the biceps tendon proximally. The nerve should be carefully mobilized from its fascial constraints around the fibula neck. As the common peroneal nerve courses into the anterior compartment the anterior fascial constraints should be released, as well as the posterior intermuscular septum. This will allow safer mobilization of the nerve. Once the nerve has safely been identified, mobilized, and tagged, the proximal fibula and fibular neck can be safely manipulated and stabilized as needed.
4. Wound closure
To avoid nerve constriction, Closure should include only skin and subcutaneous tissue.