Sinus tarsi approach to the calcaneus
1. Introduction
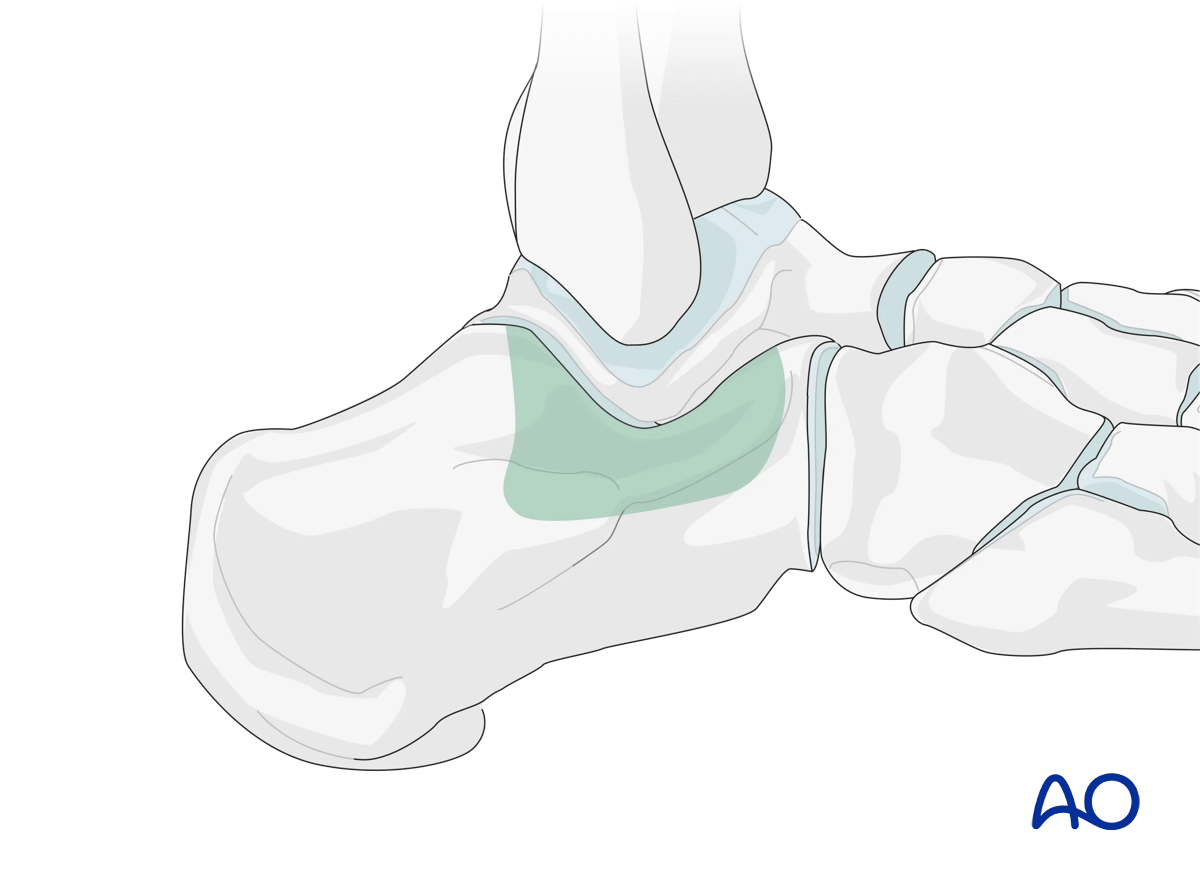
This approach is used for fixation of displaced intraarticular calcaneal fractures. It provides better visualization of the anterior aspect of the calcaneum compared to the extended lateral approach and the lateral extensile approach.
Due to this limitation of fracture exposure, it is important to have an adjunctive method, eg, external fixator, for reducing the primary fracture line.
This illustration shows the areas of the calcaneus that are visualized through this surgical approach.
2. Anatomy
Neural anatomy
Take care to protect the sural nerve.
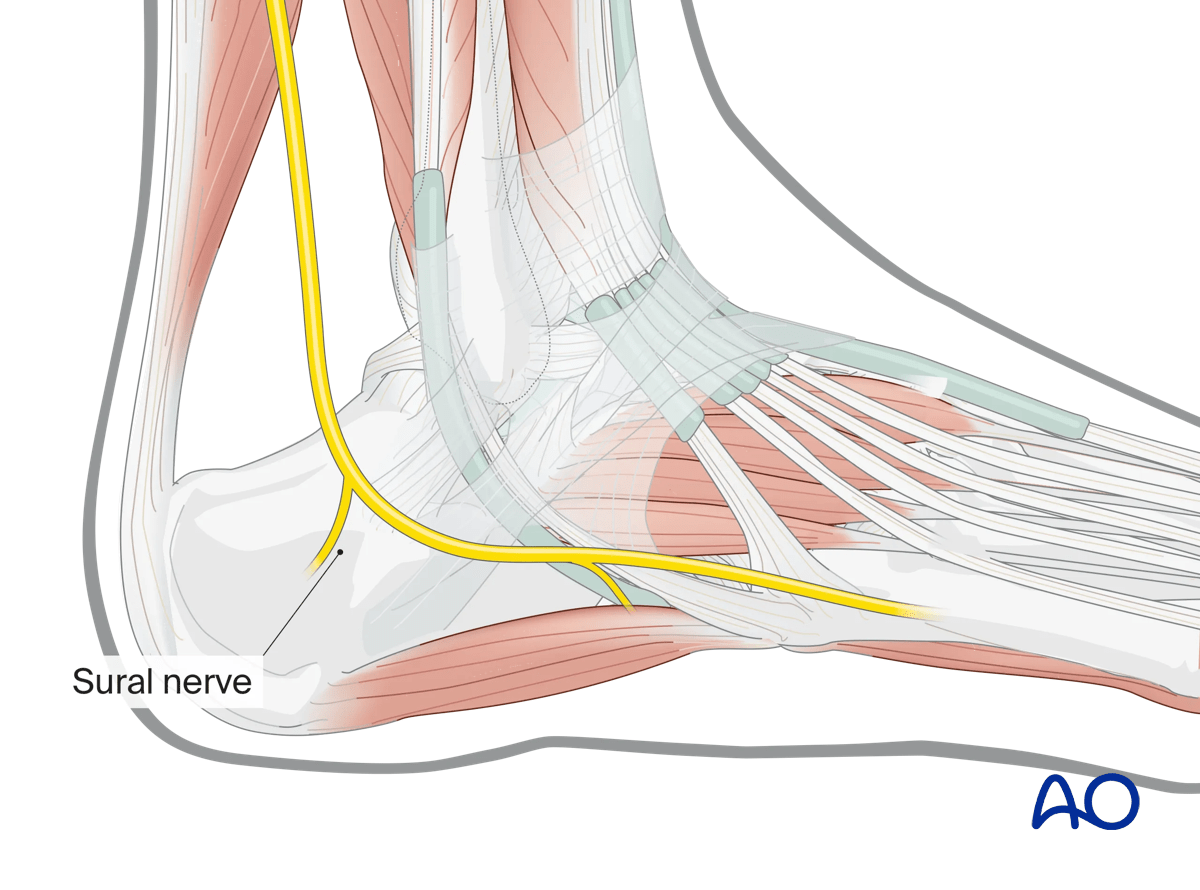
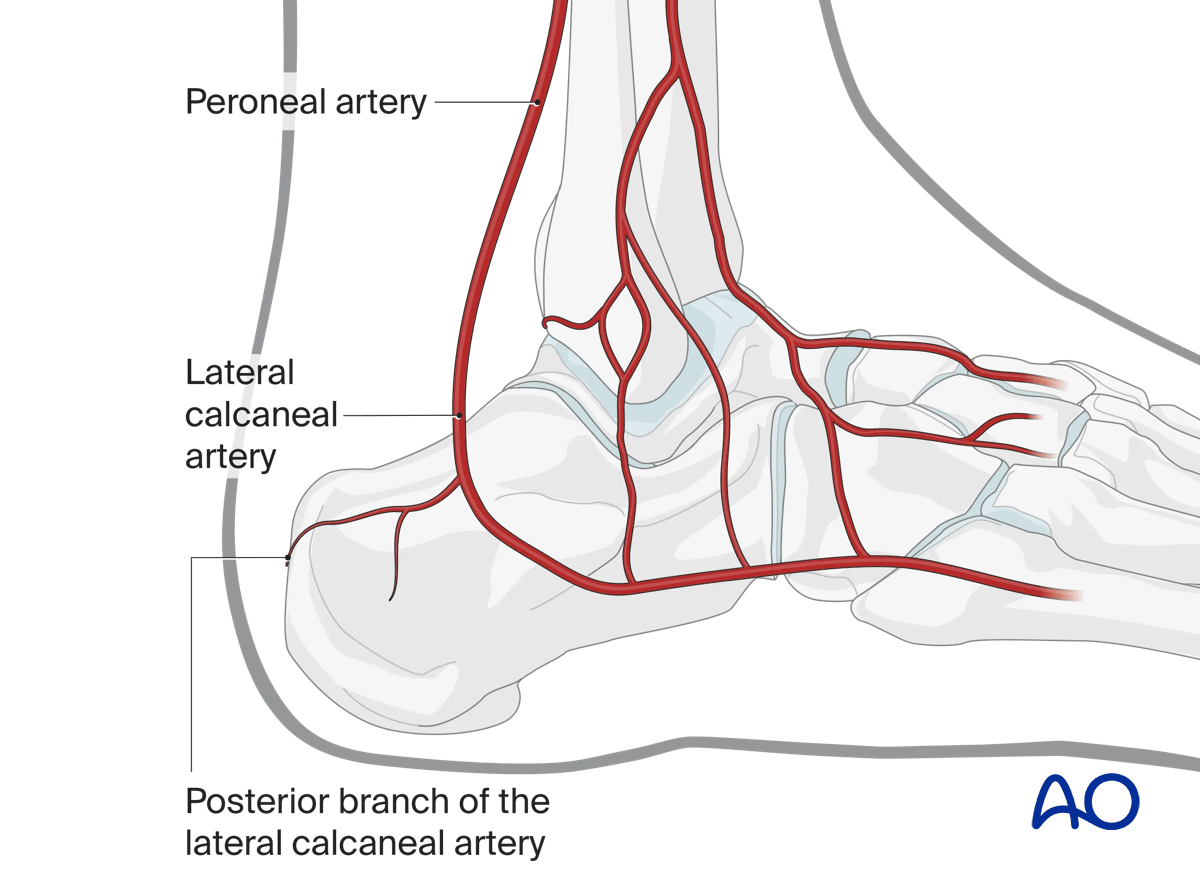
Vascular supply
The lateral calcaneal artery is responsible for most of the blood supply to this area.
If there is a need to extend the sinus tarsi approach proximally, one should avoid dissection through the deep portion of the superior peroneal retinaculum. The lateral calcaneal artery will then be protected, thus preserving the blood supply to the lateral calcaneal skin and soft tissues.
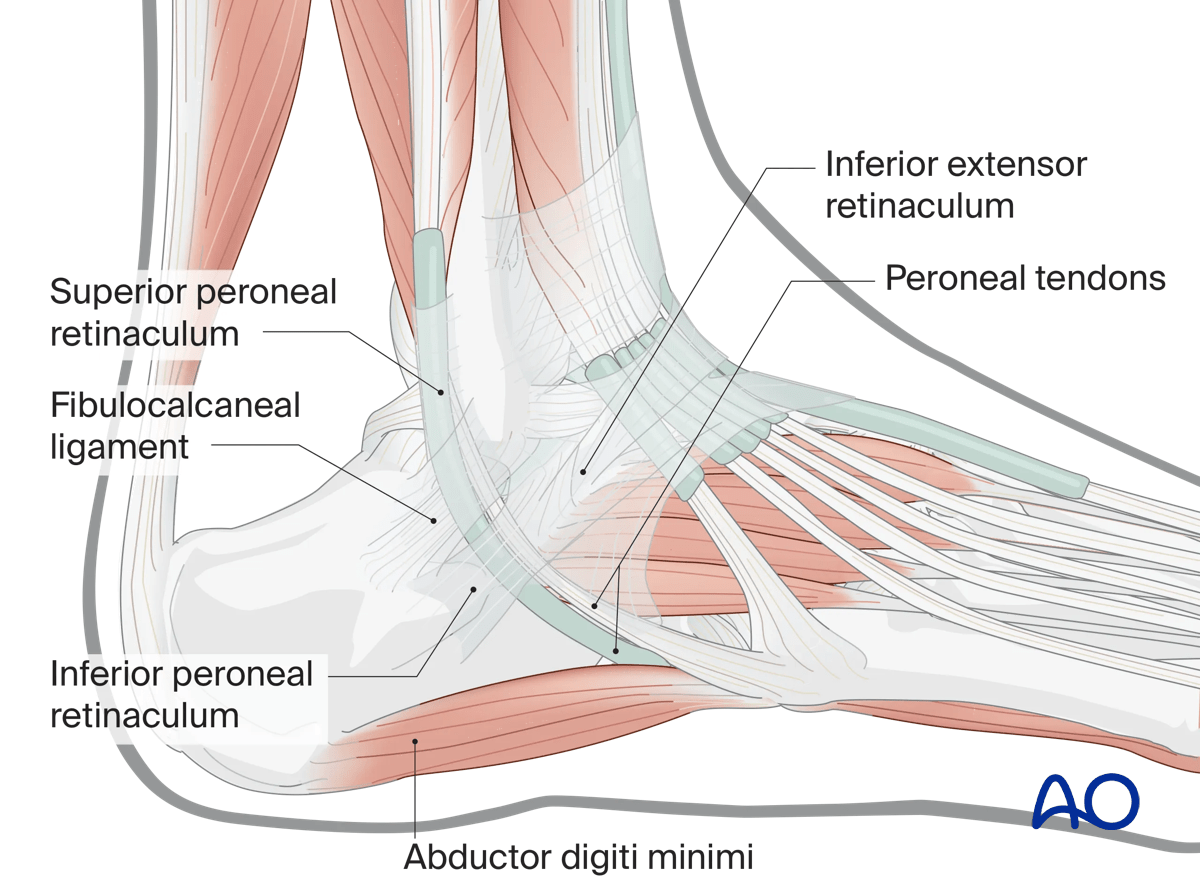
Ligaments, tendons, and muscles
The peroneal tendons are on the lateral side of the calcaneus. Note the position of the peroneal retinaculum, and the lateral collateral ligament.
3. Timing of surgery
Correct timing of surgery is an important factor in preventing local wound complication. Too early surgery may lead to skin necrosis. Therefore, patience is required to optimize the local surgical environment.
Skin blisters should be observed and carefully protected.
The image shows a foot 3 days after serious trauma, which is inappropriate for surgery.

The return of skin wrinkles to the lateral side of the foot should be used as a guide for the timing of surgery.
The image shows a foot 14 days after injury appropriate for surgery, with the “wrinkle sign” present.

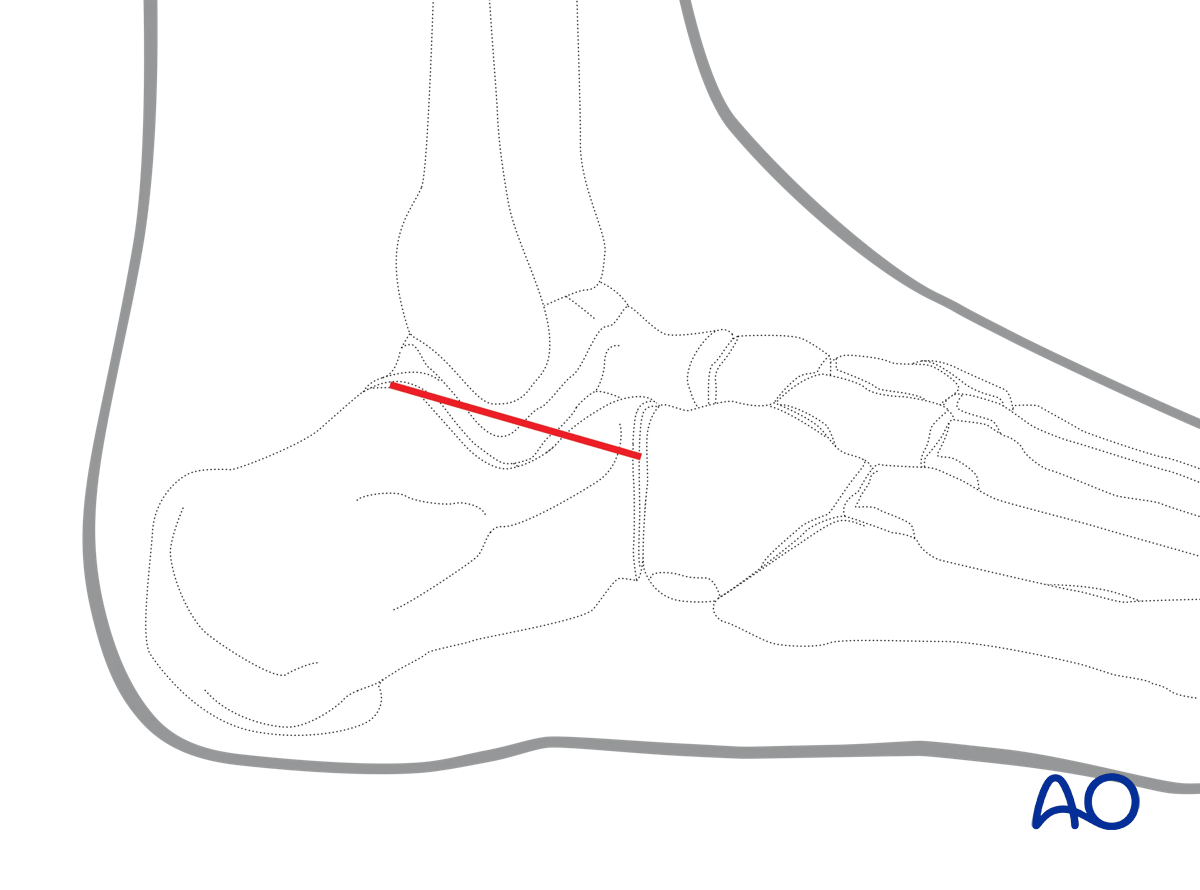
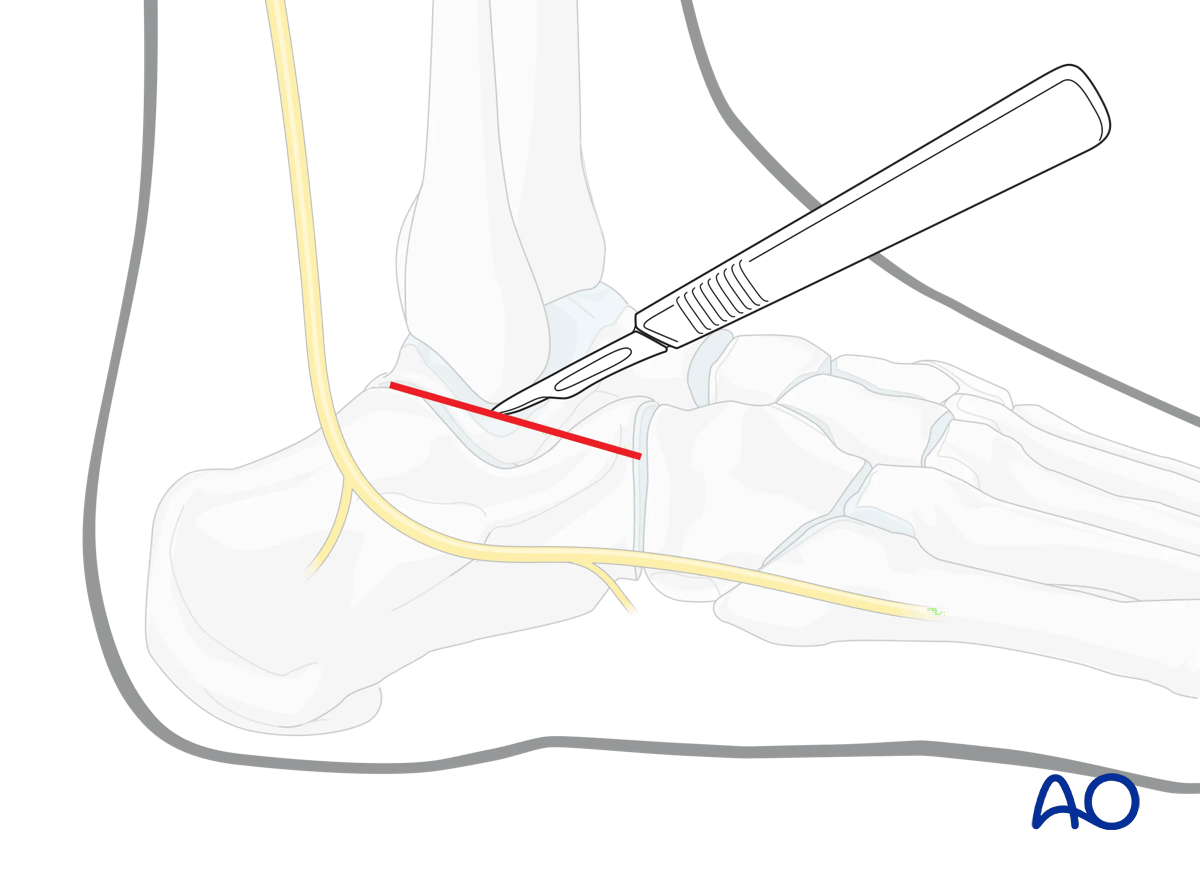
4. Incision
This approach runs from the tip of the fibula distally to the base of the fourth metatarsal base. The peroneal tendons lie inferior and posterior to the incision.
Start the incision at the tip of the fibula and extend it distally, through the skin …
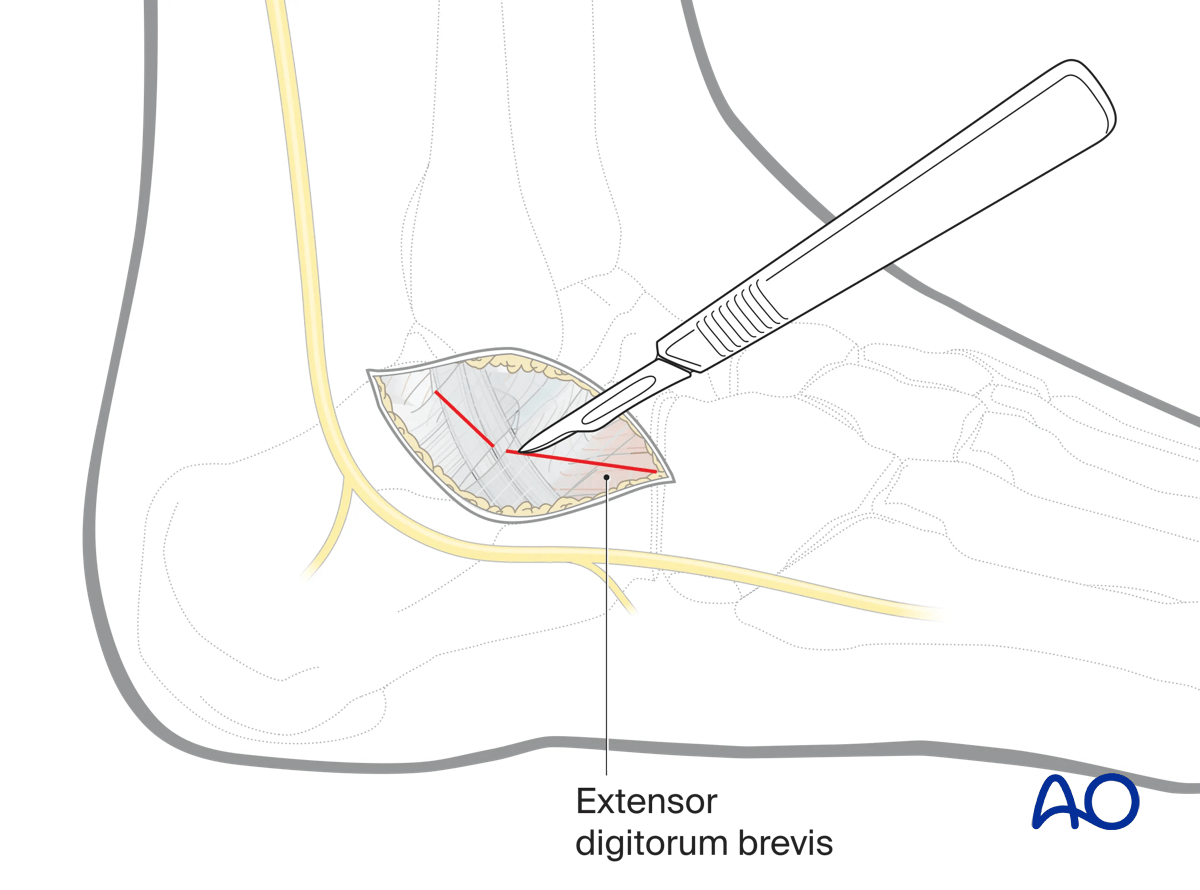
… and then through the deep fascia. Protect the tendons and the sural nerve inferiorly.
The exact orientation and length of the incision may be adjusted depending on the fracture pattern.
Part of the extensor digitorum brevis may be reflected.
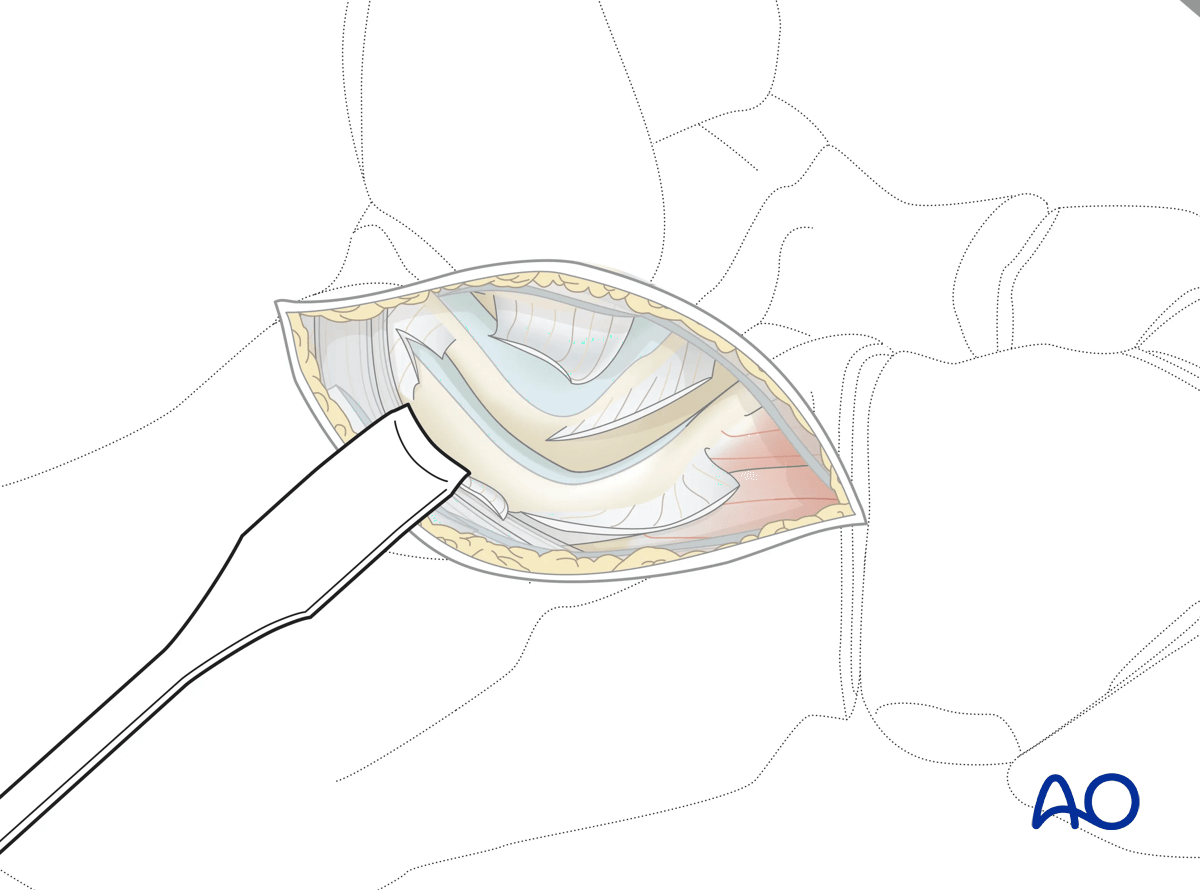
5. Approaching the subtalar joint
Enter the joint capsule and expose the subtalar joint.
This small incision allows for direct visualization of the subtalar joint. The quality of reduction can be assessed. The internal fixation construct can be inserted through this incision; it can be lengthened as needed.
Subtalar arthroscopy can assist in accurate joint reduction.
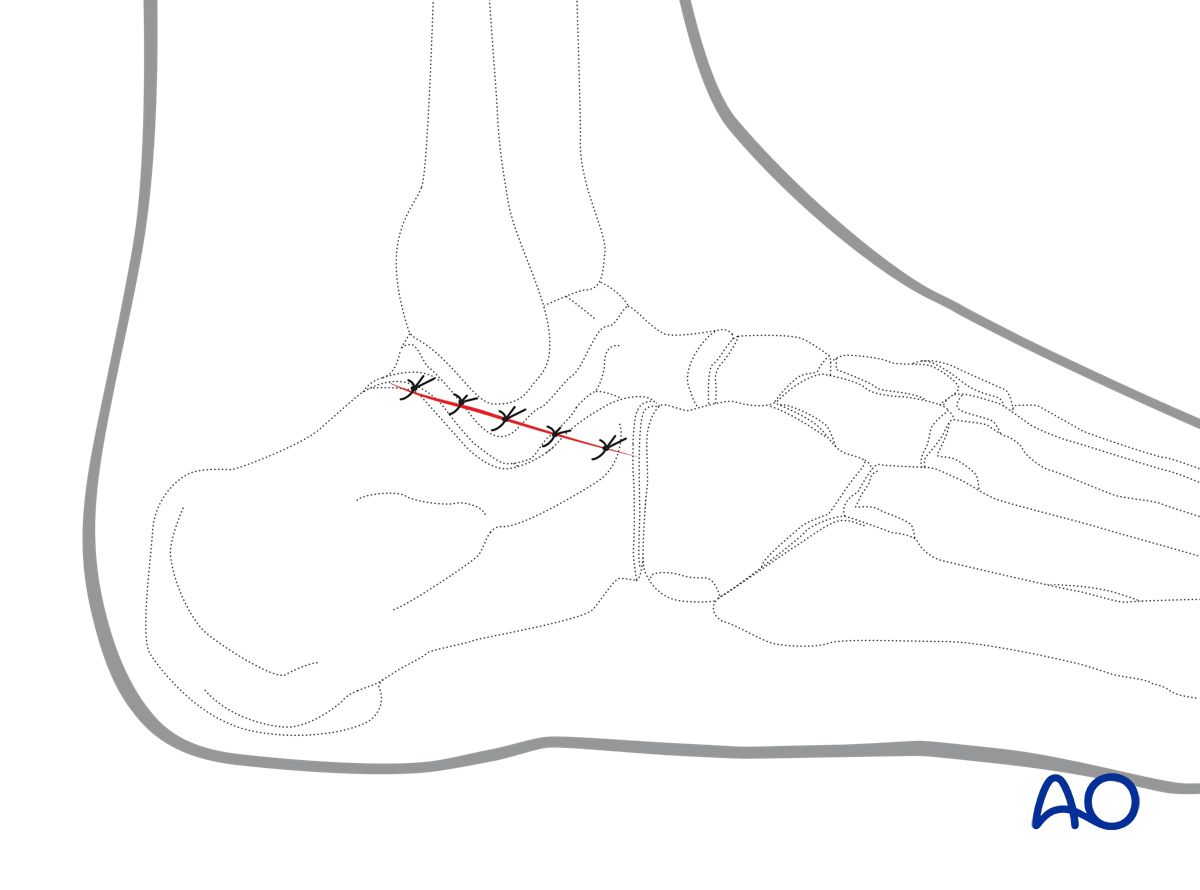
6. Wound closure
The retracted extensor digiti minimi may be replaced.
The deep layer can be closed with absorbable sutures.
The skin is closed either with a continuous subcuticular suture or an interrupted skin suture.