MIO posterior approach to the calcaneus
1. Introduction
This approach is used for minimally invasive reductions and percutaneous fixation of displaced intra- or extraarticular calcaneal fractures. It is common for this approach to be undertaken when the calcaneal fracture is of a simpler fracture pattern.
It is part of the vertical limb of the extended lateral approach.
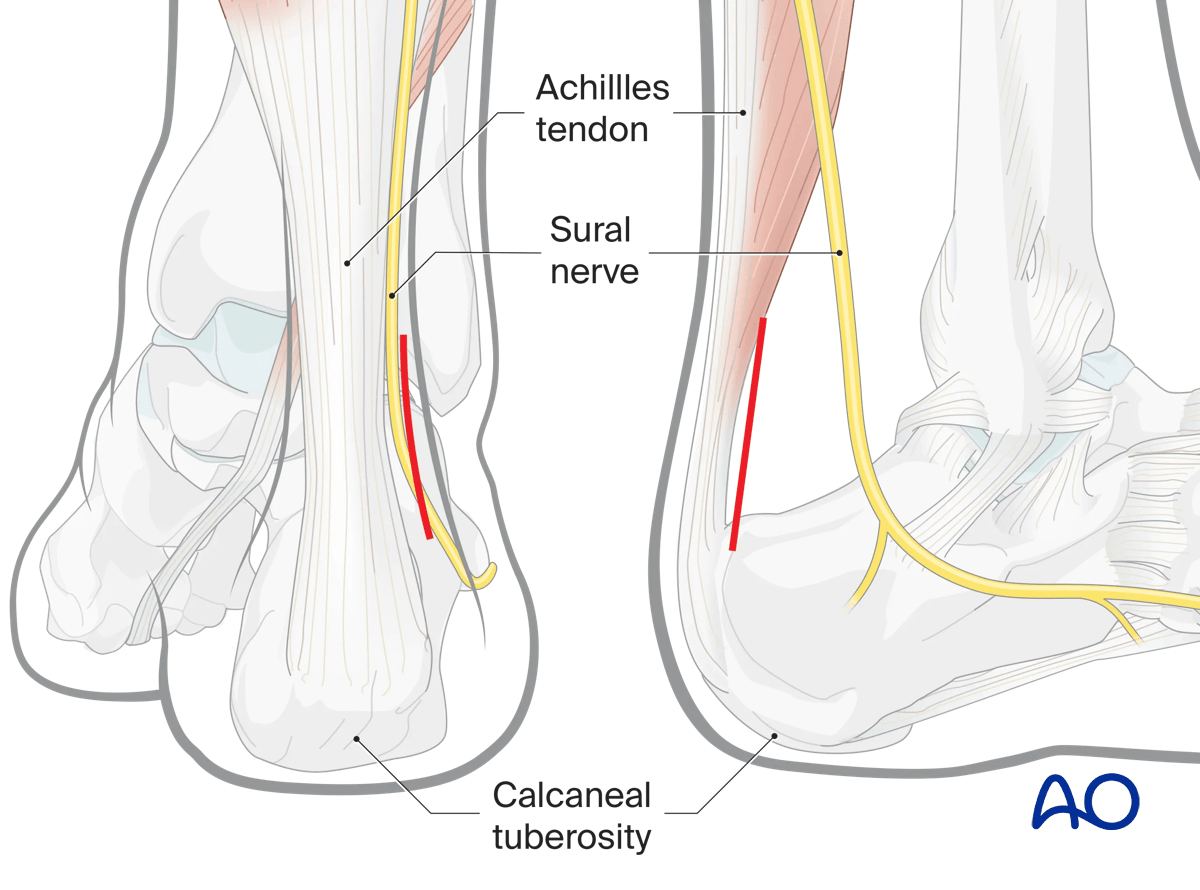
Optionally, the incision may be performed medial to the Achilles tendon. Care must be taken to avoid damage to the neurovascular bundle.
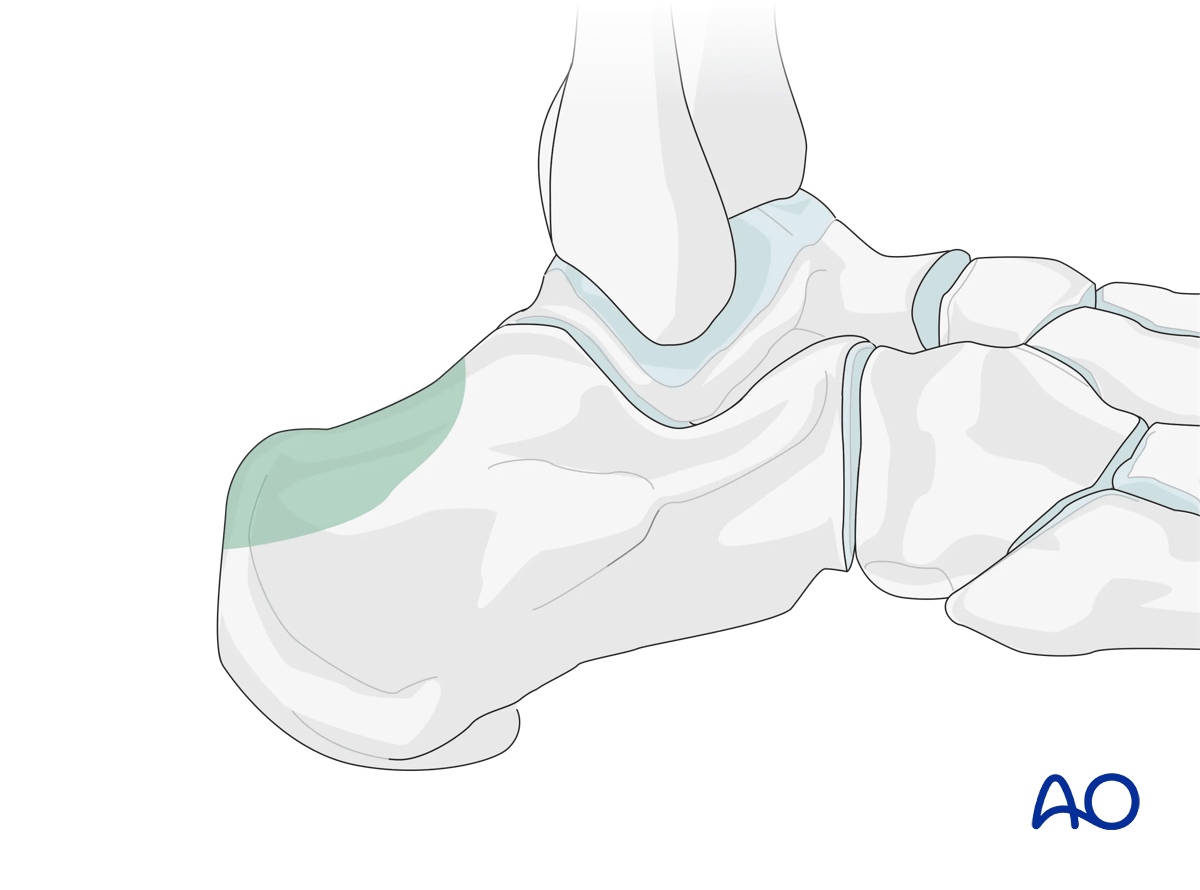
This illustration shows the areas of the calcaneus that are visualized through this surgical approach.
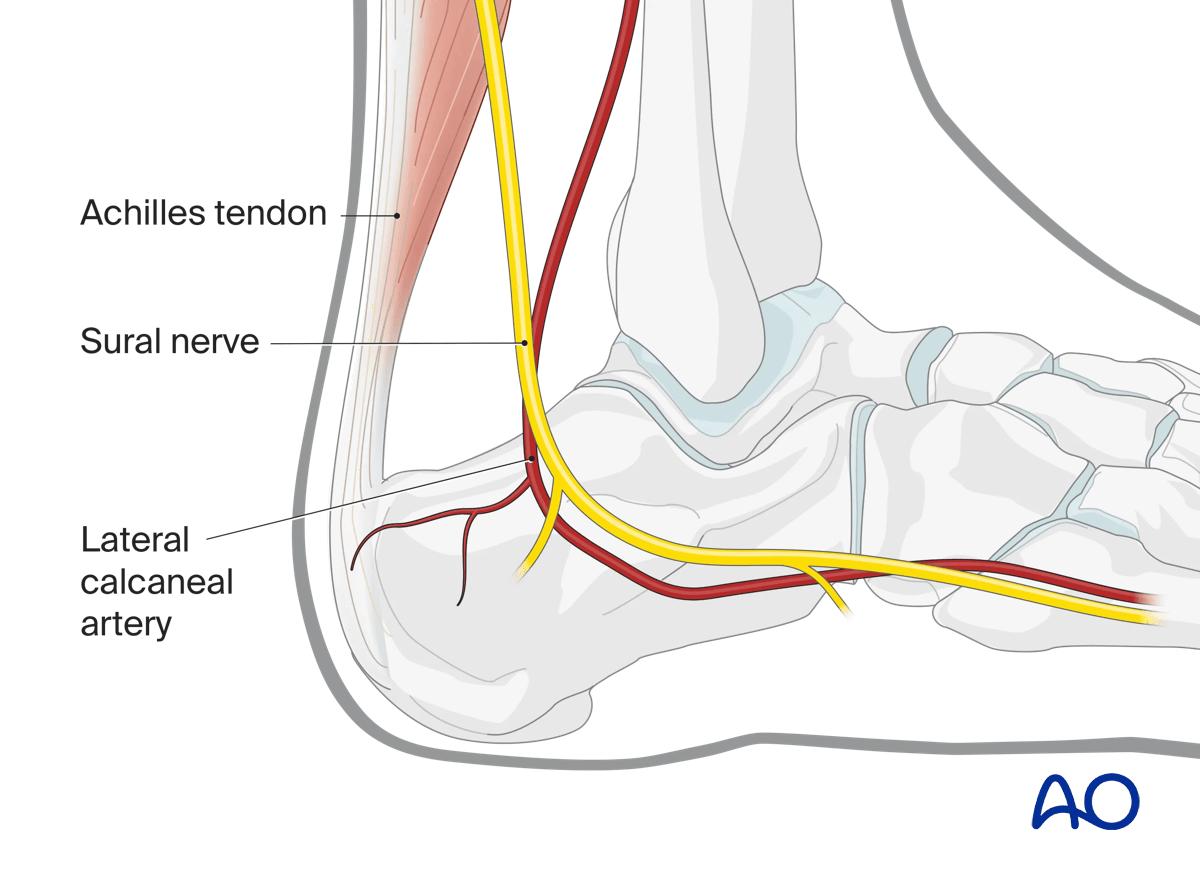
2. Anatomy
The lateral calcaneal artery is responsible for most of the blood supply to this area.
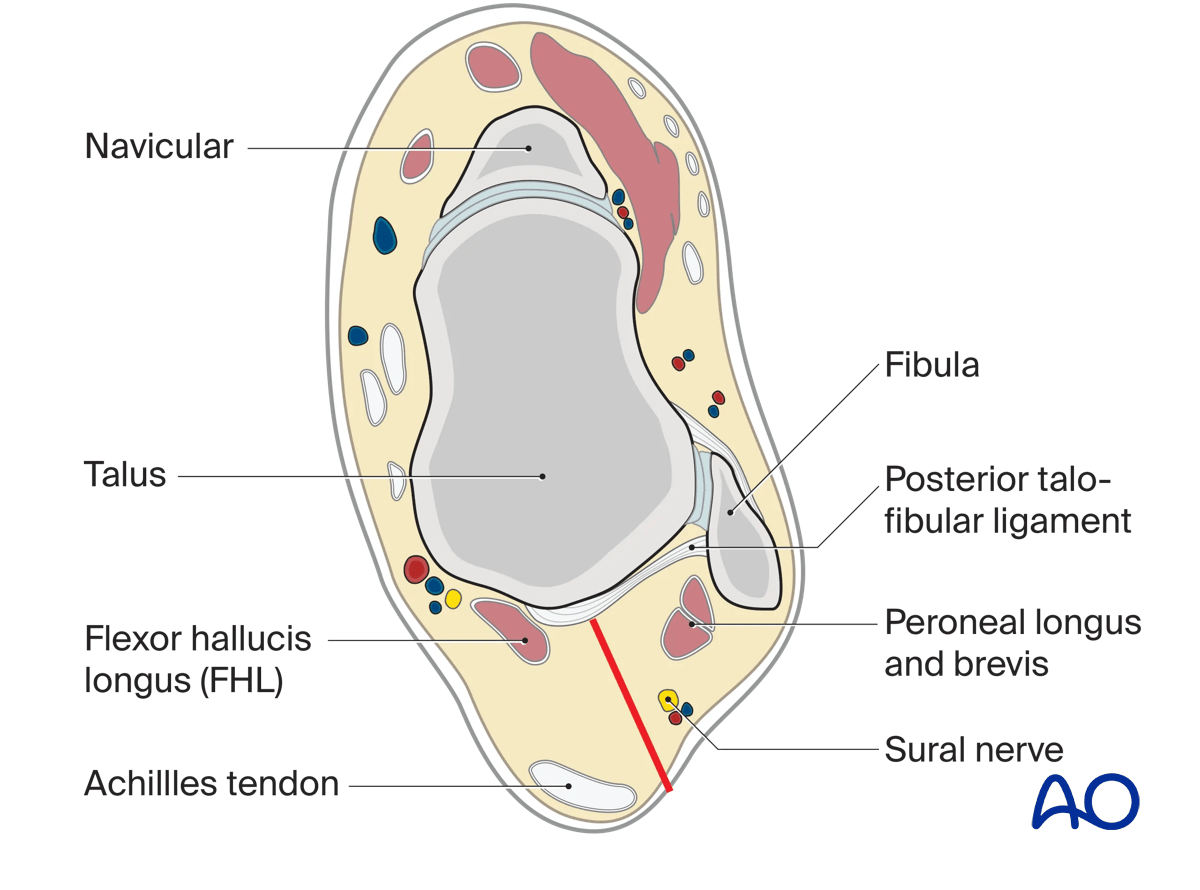
This approach respects the Achilles tendon and sural nerve, and lateral calcaneal artery (posterior peroneal artery).
3. Timing of surgery
Correct timing of surgery is the most important factor in preventing local wound complication.
Sometimes a fracture may endanger the skin like a tuberosity fracture shown in this image.
In such cases, reduction must be undertaken urgently, and the incision used may be modified.

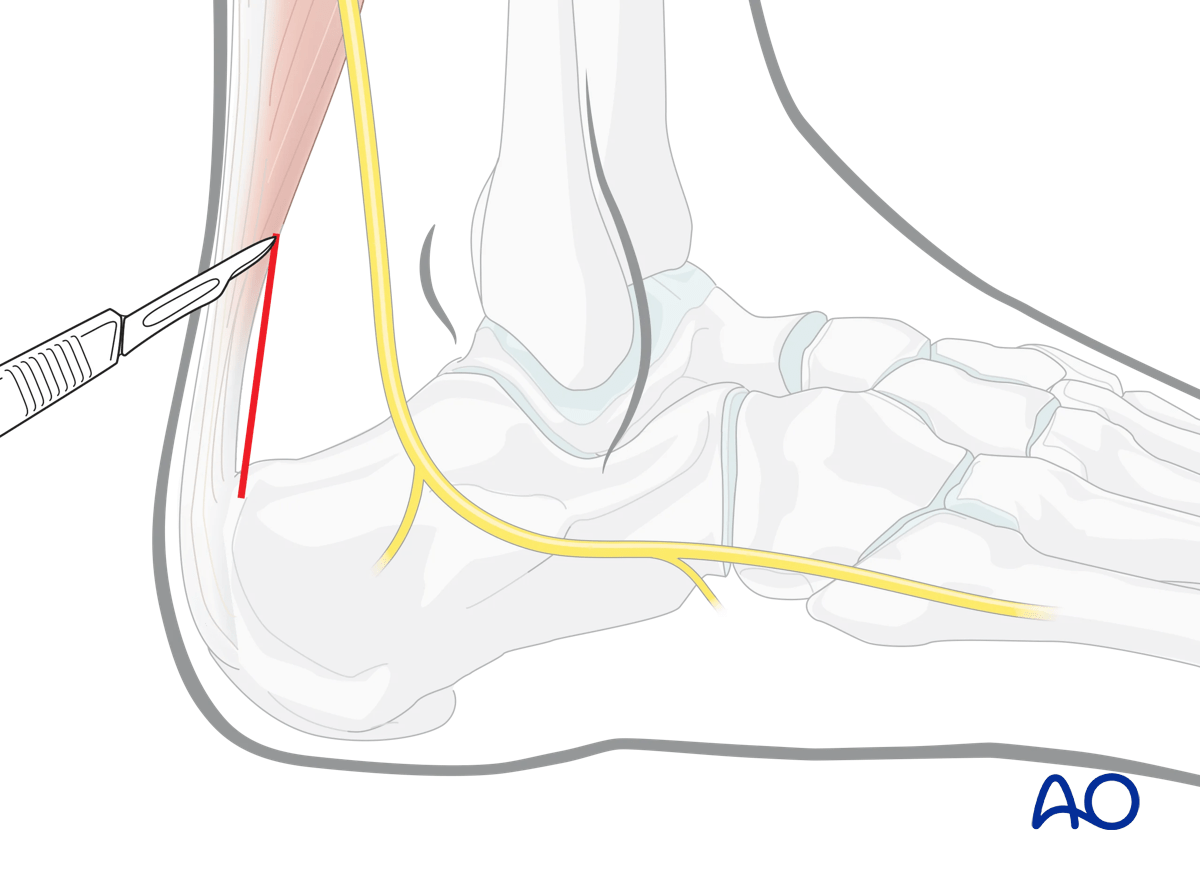
4. Incision
The landmarks for this incision are the lateral aspect of the Achilles tendon and the calcaneal tuberosity. The incision should not be over the Achilles tendon.
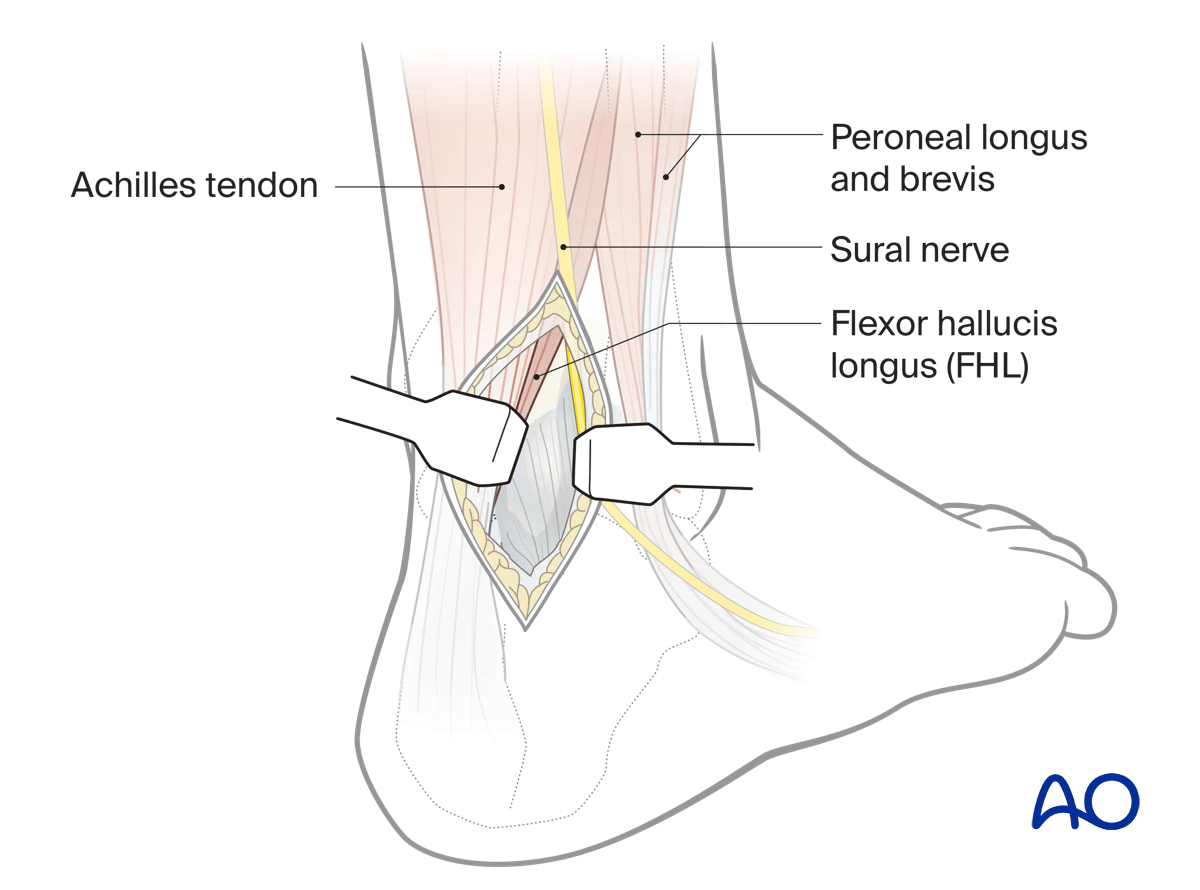
Deepen the incision lateral to the paratenon of the Achilles tendon, then through the fat of the pre-Achilles space down to the superior border of the calcaneum.
Medially, the belly of FHL protects the posterior tibial neurovascular bundle.
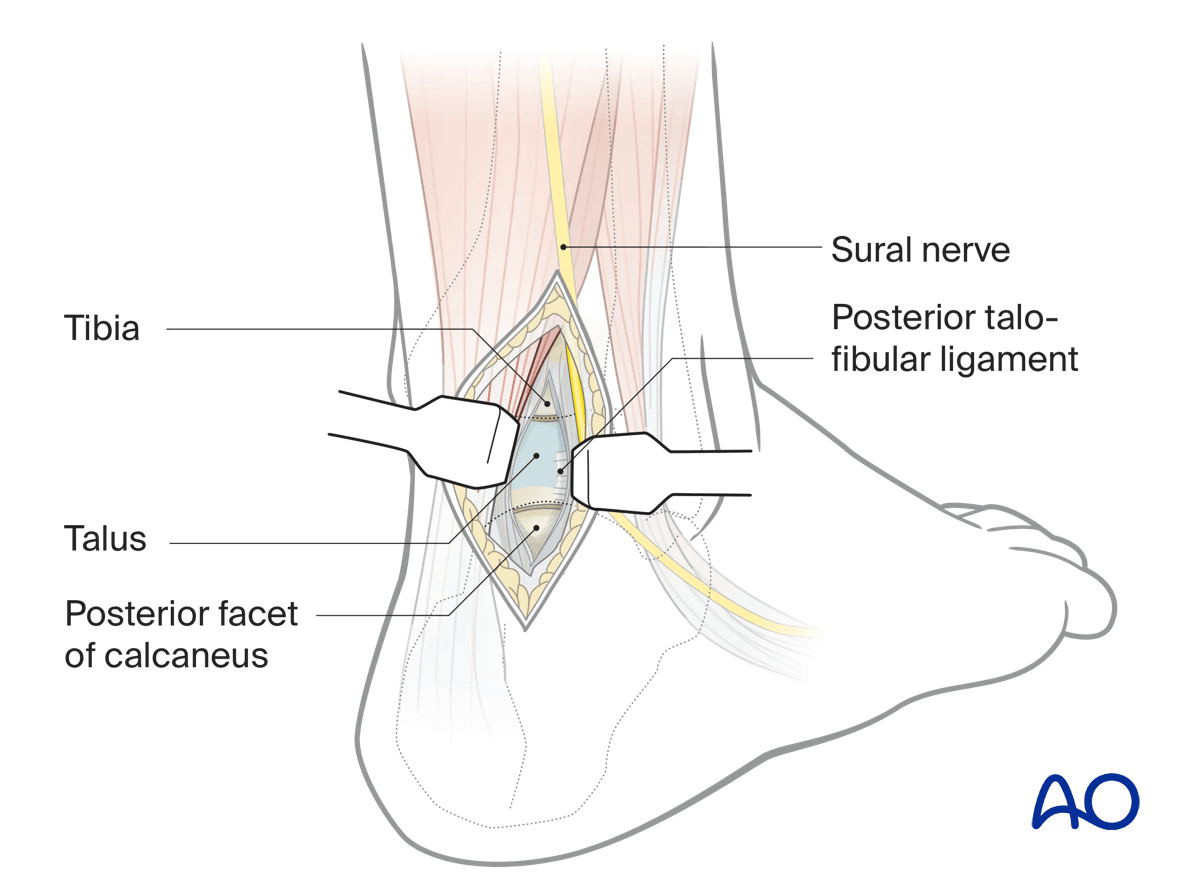
Incise the capsules of the ankle and subtalar joint vertically. This will expose superiorly the distal tibia and inferiorly the calcaneus with the talar body between them.
The use of a distractor between the tibia and the calcaneum will increase the exposure.
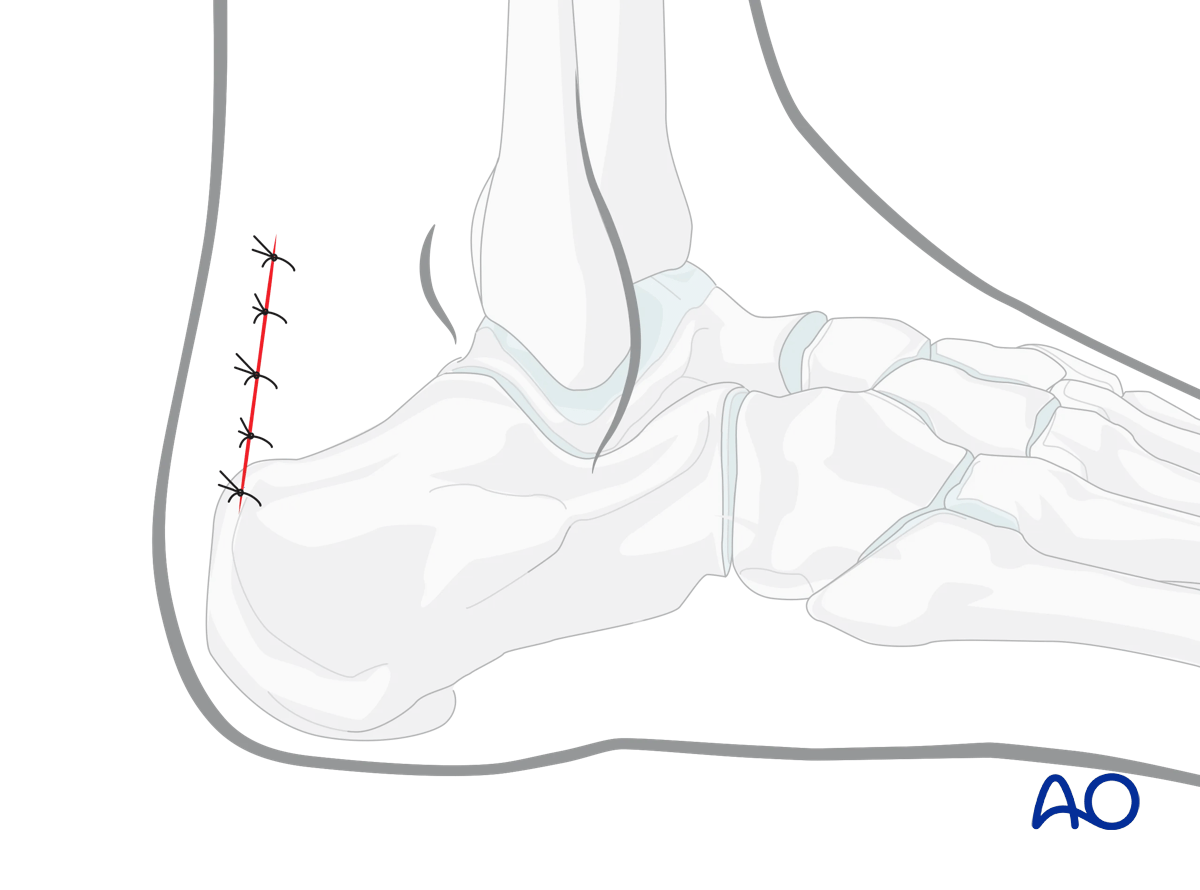
5. Wound closure
The deep tissues are closed with an absorbable suture.
For skin closure, either a continuous subcuticular absorbable suture may be used or an interrupted suture.