Medial approach to the calcaneus
1. Indications
The medial approach to the calcaneus may be used for displaced fractures of the sustentaculum tali or for direct exposure of the medial wall.
Almost all calcaneal fractures are best approached laterally or posteriorly, but sustentacular fractures, which make up a small percentage (<10%) of calcaneal fractures, may be approached through the medial side of the hindfoot.
This approach is often helpful to assist in debriding open fractures of the calcaneus, as most open fractures occur over the sustentacular fragment medially when it pierces the skin.
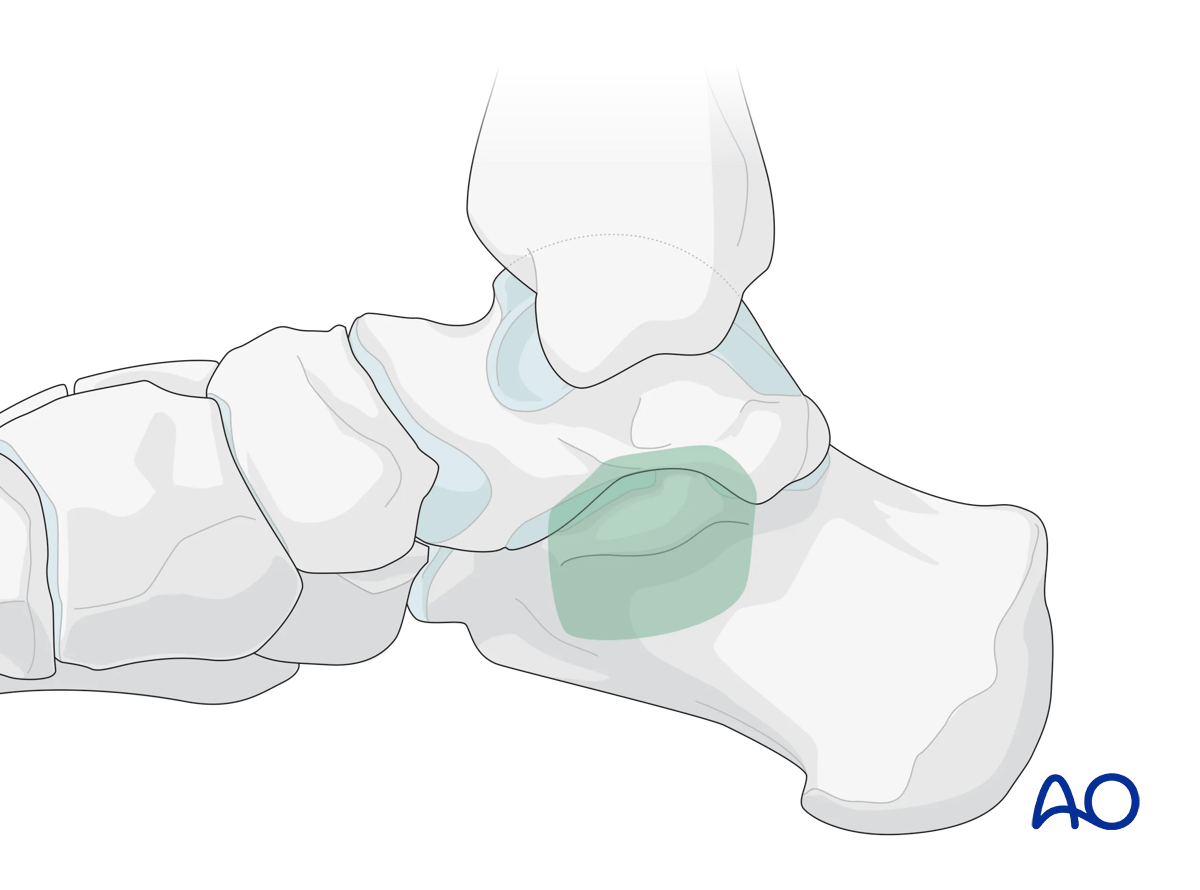
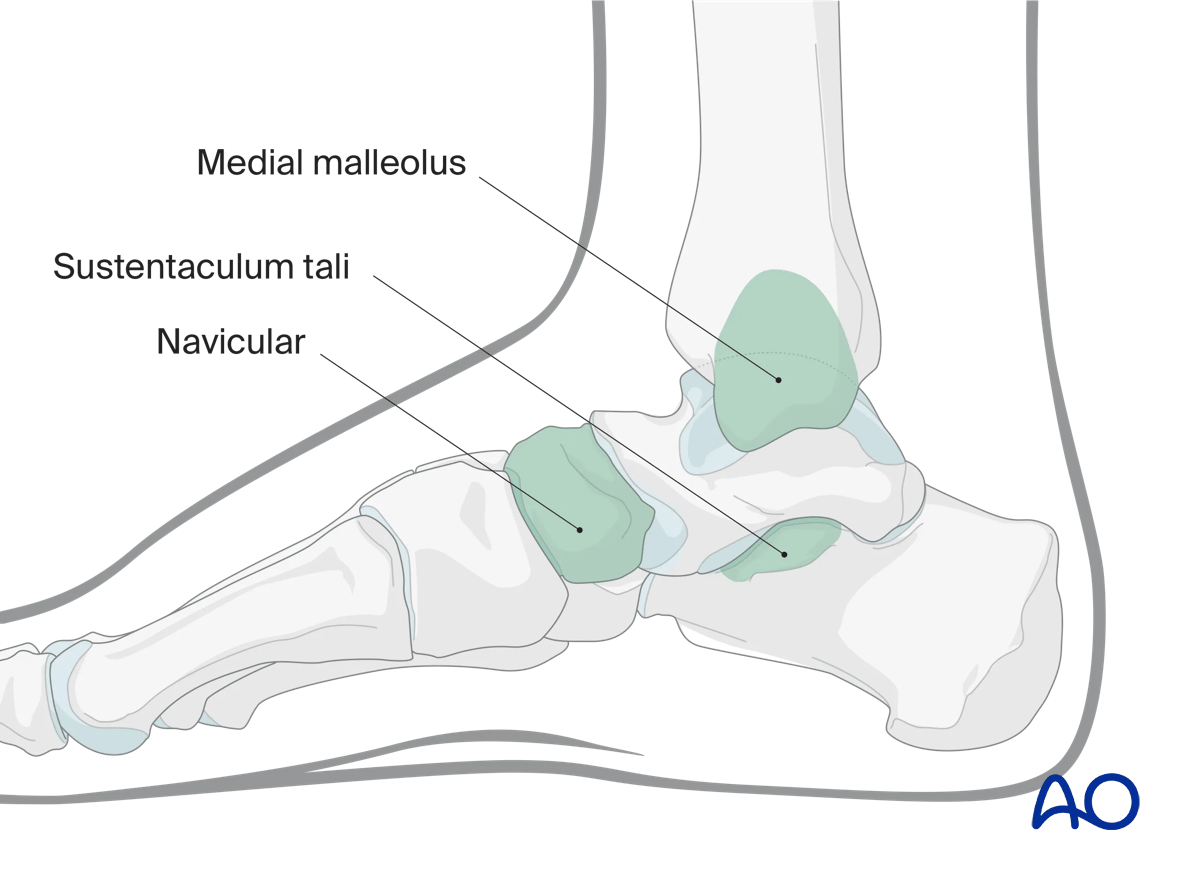
This illustration shows the areas of the calcaneus that are visualized through this surgical approach.
2. Anatomy
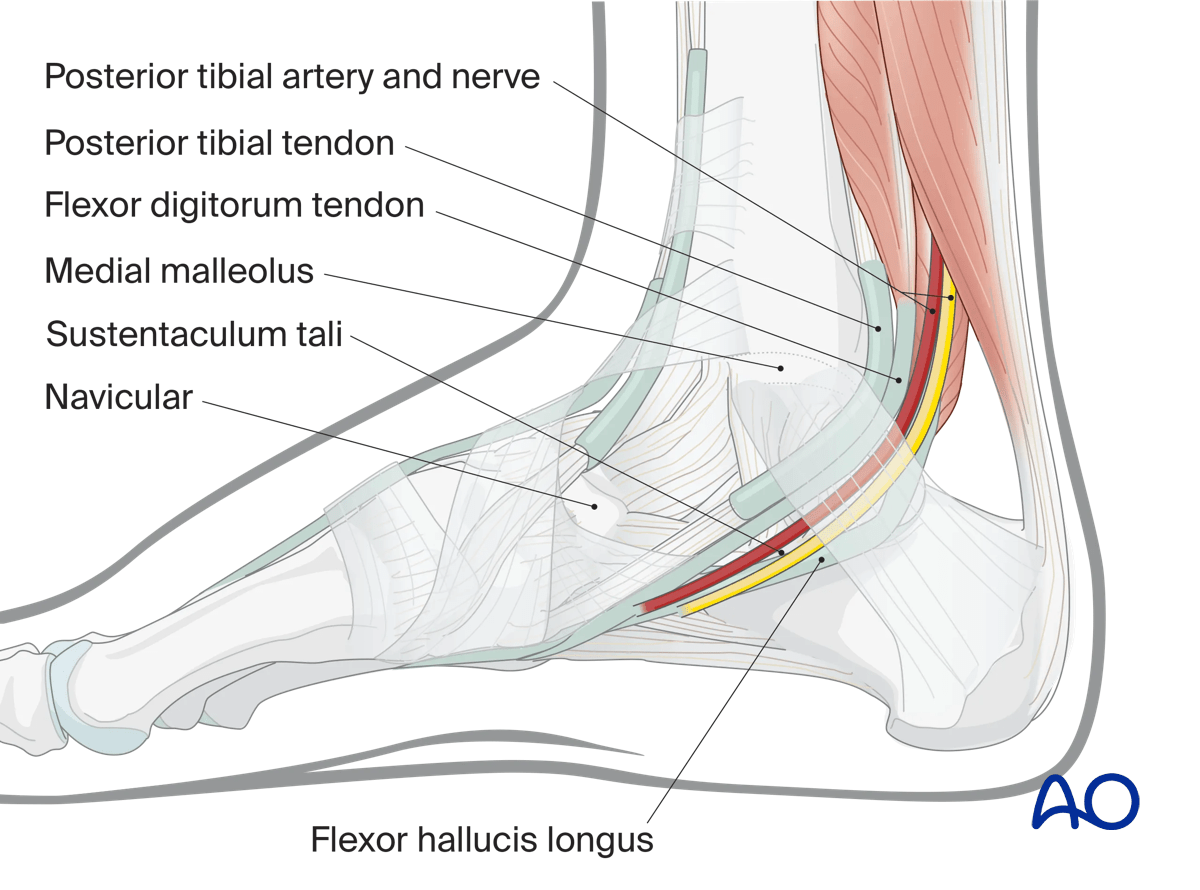
Key anatomic structures that relate to this approach include:
- Medial malleolus
- Navicular
- Sustentaculum tali
- Posterior tibial artery, vein, and nerve
- Posterior tibial tendon
- Flexor digitorum tendon
- Flexor hallucis longus tendon
3. Incision
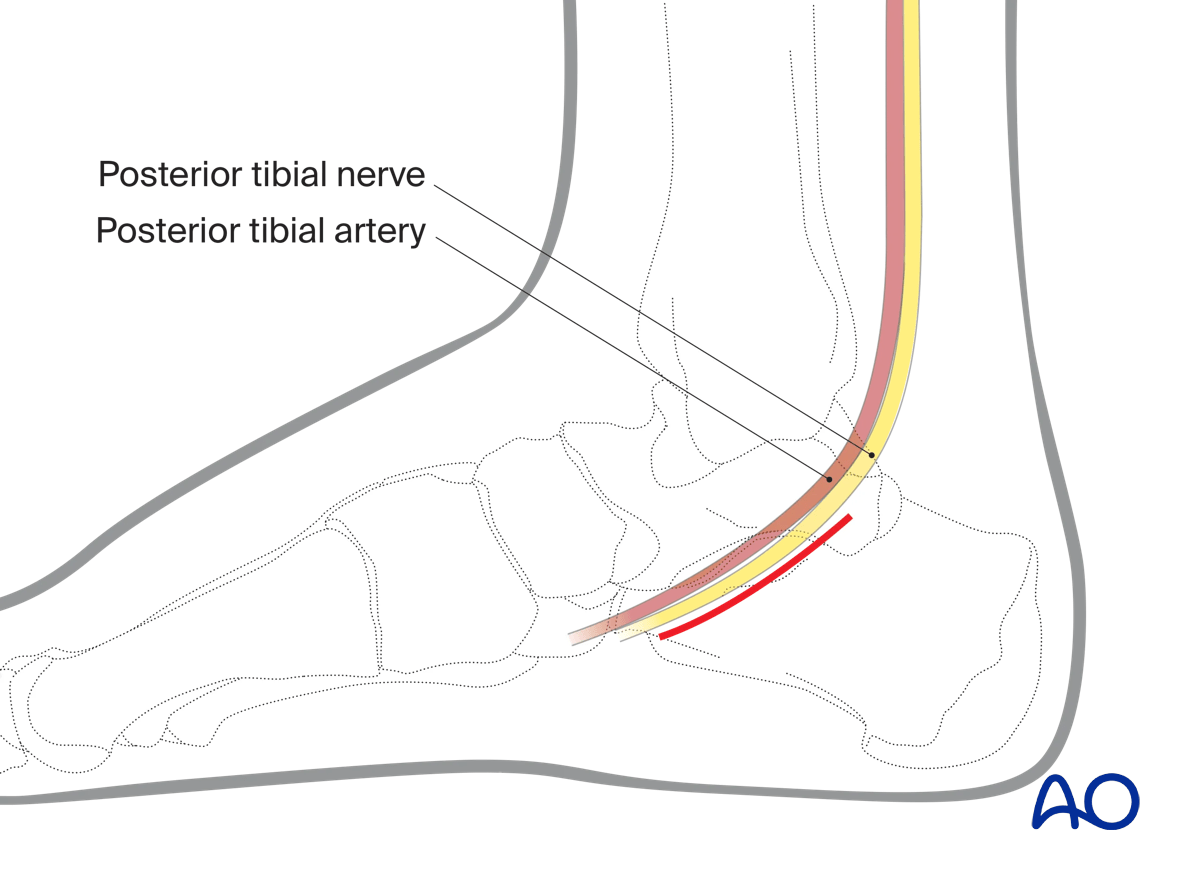
Palpable landmarks
The sustentaculum tali can be palpated about two finger breadth inferior to the medial malleolus. It is roughly in line with the medial process of the navicular.
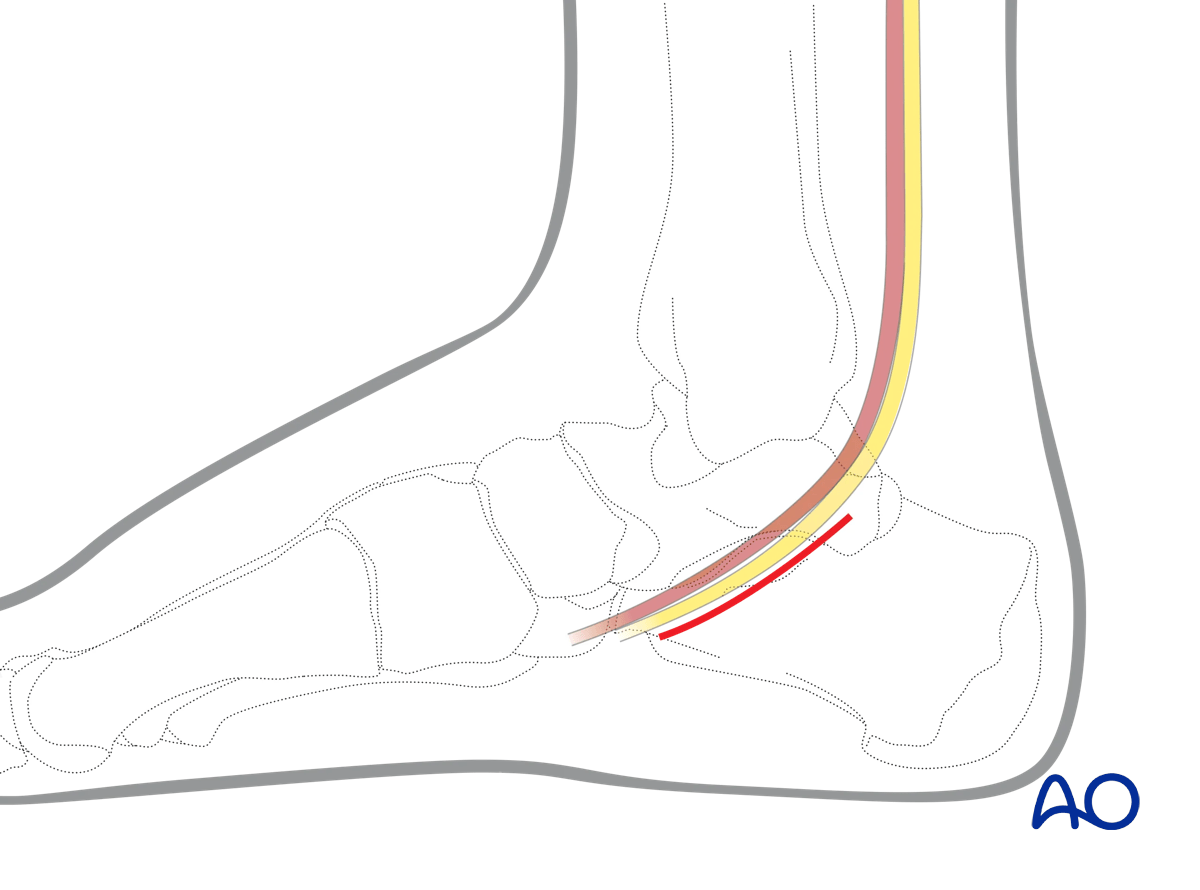
Skin incision
The incision parallels the neurovascular bundle from just behind the medial malleolus to the proximal end of the navicular.
The center of the incision is 2 cm beneath the medial malleolus.
To achieve adequate visualization of the sustentaculum, it needs to be about 5 cm in length.
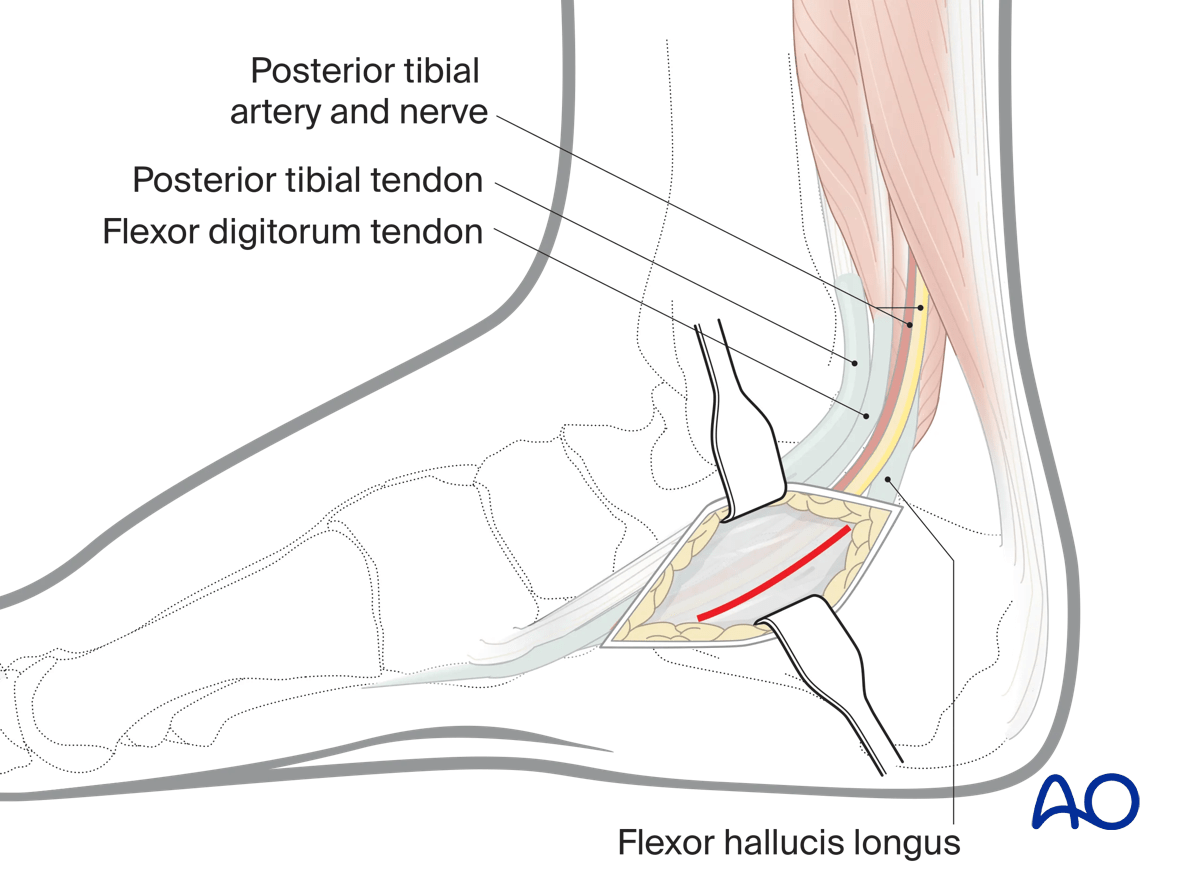
Superficial dissection
Once beneath the skin, incise the flexor retinaculum and identify the posterior tibial tendon and flexor digitorum longus tendon, the neurovascular bundle and the flexor hallucis longus tendon. The interval to develop is between the neurovascular bundle, specifically the posterior tibial nerve and the flexor hallucis longus tendon, which is retracted plantar wards. Palpate for the prominence of the sustentaculum. It is immediately above the flexor hallucis longus tendon.
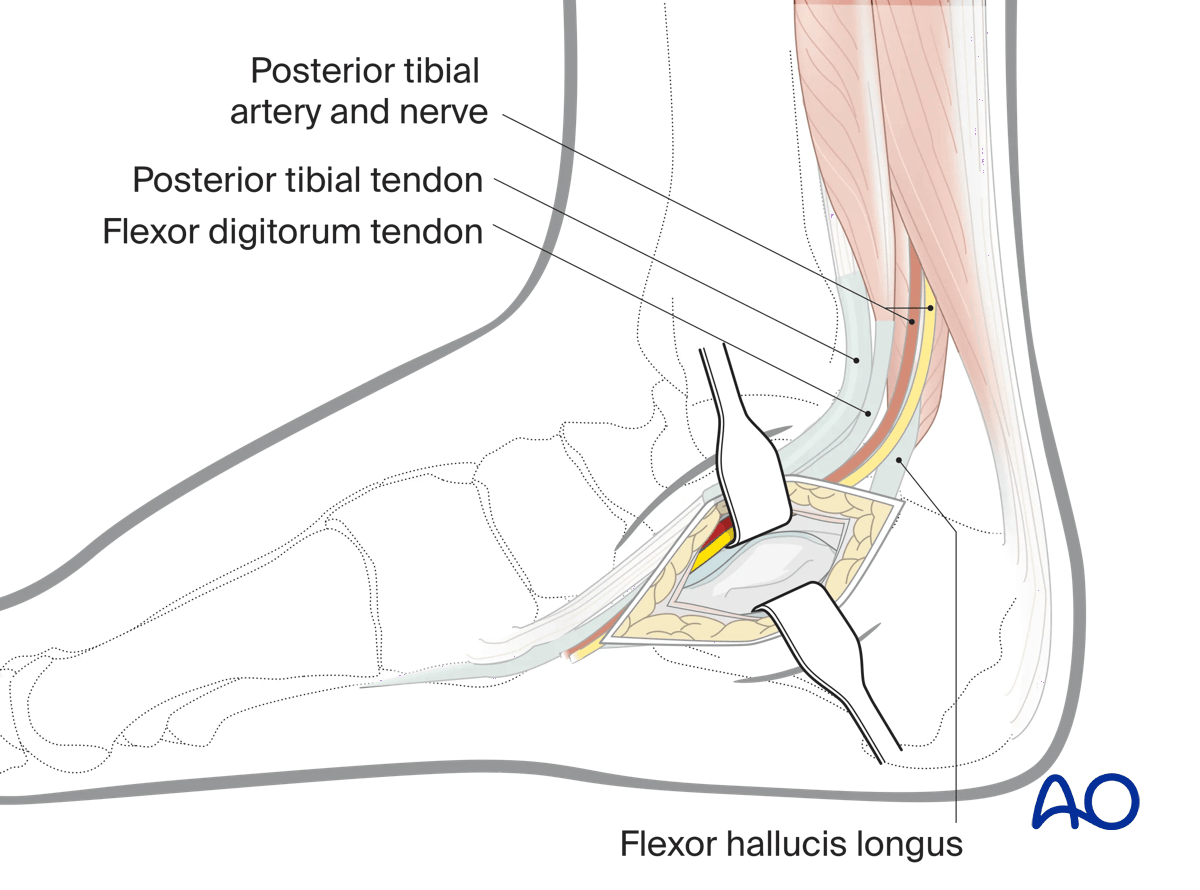
Deep dissection
Dissection deep to the flexor hallucis longus tendon reveals the sustentaculum tali and the medial wall of the calcaneus.
Image intensification can be used to verify the location of the sustentaculum tali.
Depending on the exact configuration of the fracture, multiple windows may be required either side of the tendon and neurovascular bundle.
The tibiocalcaneal portion of the deltoid ligament should be left intact to avoid medial instability and damage to the blood supply to the talar body via the deltoid branches.
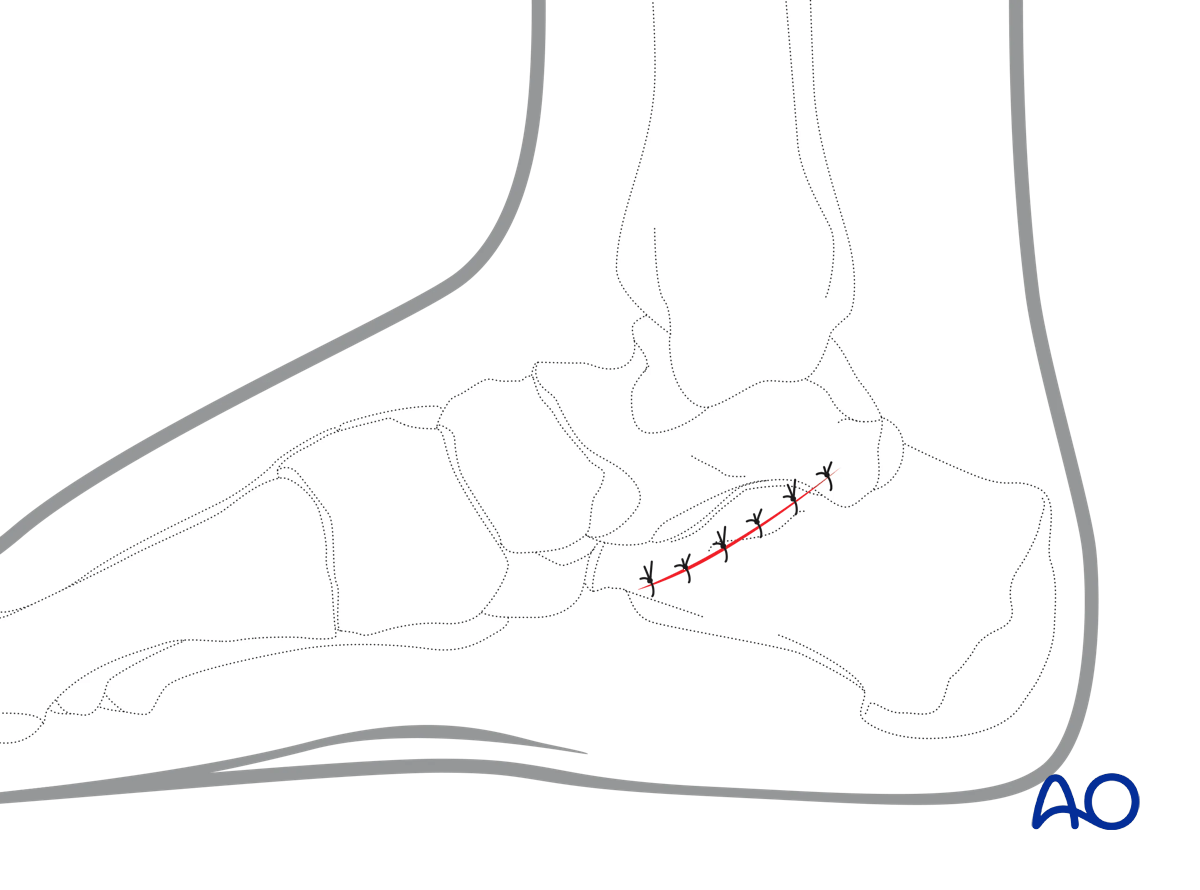
4. Wound closure
This approach is closed with interrupted subcutaneous absorbable sutures and continuous subcuticular sutures or interrupted skin sutures.