Extended lateral approach to the calcaneus
1. Introduction
The extended lateral approach to the calcaneus is a versatile approach that can be used for open reduction and internal fixation of all calcaneal fractures. It can also be used for a wide range of elective hindfoot surgery.
It is a technically demanding approach, and very careful attention must be paid to the position of the skin incisions. When performing deep dissection, some of the lateral wall bone fragments should be kept attached to the cutaneous flap.
Correctly undertaken, sural nerve damage does not occur and soft tissue problems are mostly limited to minor tip necrosis in high energy cases. Operative treatment of calcaneal fractures via either an extended lateral approach or sinus tarsi approach can achieve comparable postoperative radiographic outcomes.
The extended lateral approach is significantly more invasive but provides more direct visualization of the entire fracture which may allow improved reduction of severe cases.
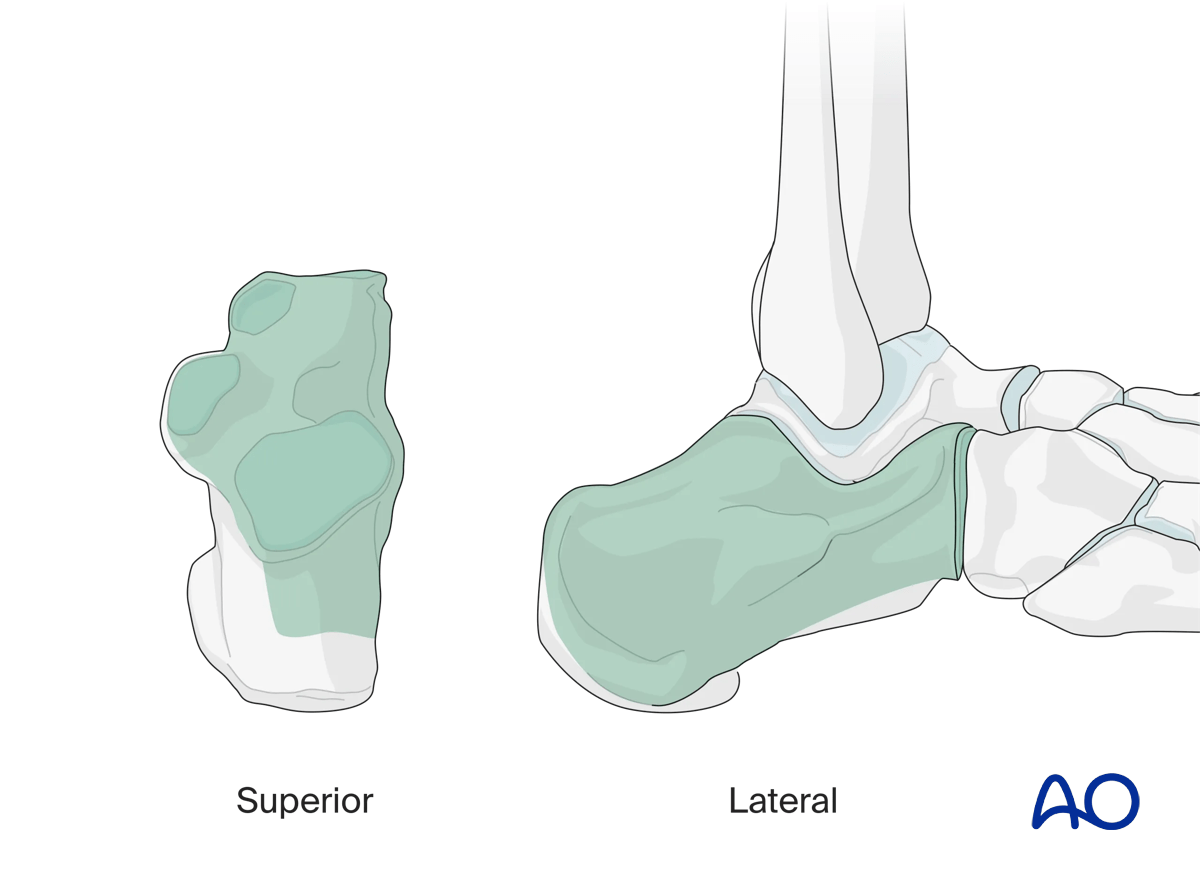
This illustration shows the areas of the calcaneus that are visualized through this surgical approach.
2. Anatomy
Neurovascular structures
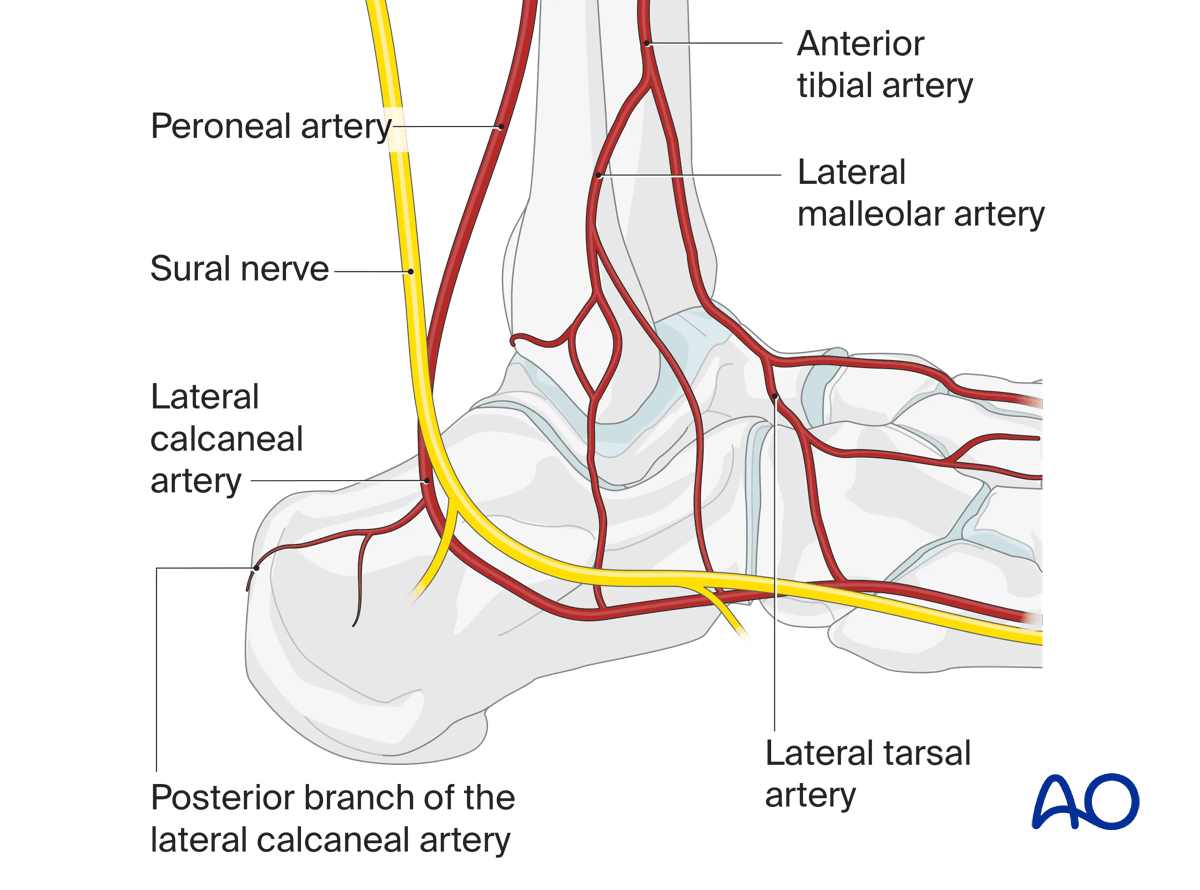
It is essential to understand the vascular supply to the soft tissues of the lateral hindfoot to avoid wound healing problems.
The vascular supply to the soft tissues of the lateral side of the hindfoot is the lateral calcaneal artery (posterior peroneal artery), which is usually the terminal branch of the peroneal artery. Superiorly, there are anastomoses with the lateral malleolar artery, a branch of the anterior tibial artery and distally, there are anastomoses with the lateral tarsal artery which is a branch of the dorsalis pedis artery.
If the incision is correctly undertaken, the sural nerve is not in danger except possibly in the very superior part of the vertical incision which is why this should be towards the midline posteriorly.
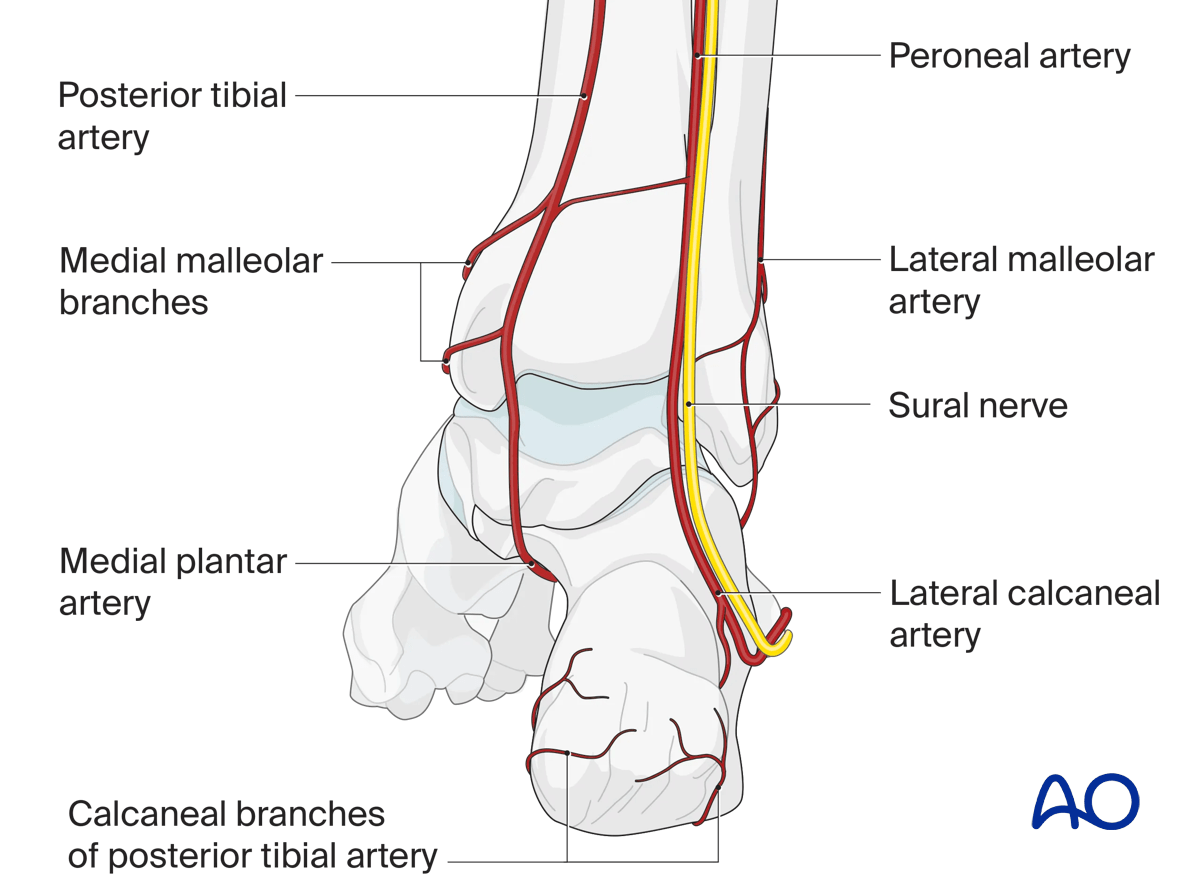
Posterior aspect with neurovascular structures
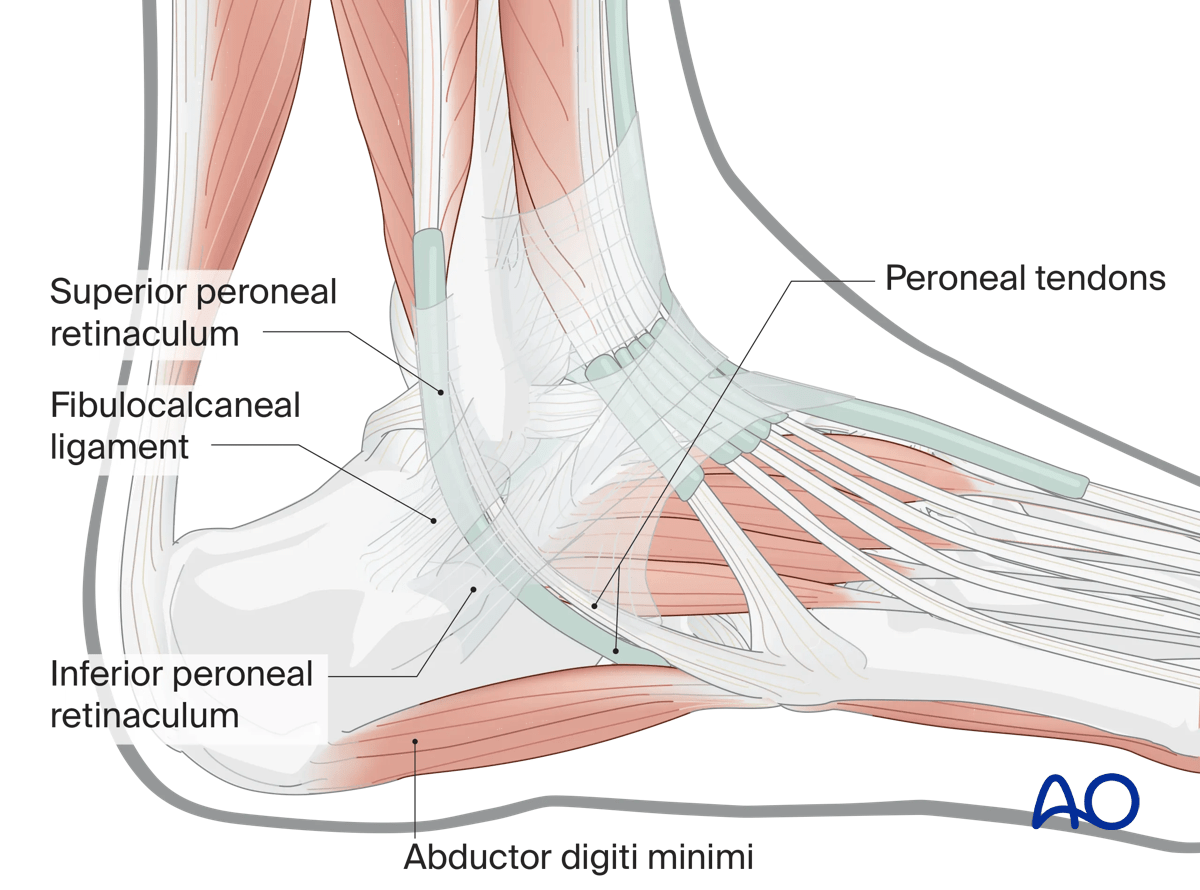
Ligaments, tendons, and muscles
In raising the lateral flap, which is a lateral calcaneal artery (posterior peroneal artery) flap, dissection is strictly subperiosteal, elevating the lateral collateral ligament of ankle and the inferior peroneal retinaculum with the subperiosteal flap.
3. Timing of surgery
Correct timing of surgery is an important factor in preventing local wound complication. Too early surgery may lead to skin necrosis. Therefore, patience is required to optimize the local surgical environment.
Skin blisters should be observed and carefully protected.
The image shows a foot 3 days after serious trauma, which is inappropriate for surgery.

The return of skin wrinkles to the lateral side of the foot should be used as a guide for the timing of surgery.
The image shows a foot 14 days after injury appropriate for surgery, with the “wrinkle sign” present.
The eventual incision will be at the junction of the sole and lateral skin and well distal to the area of bruising.

4. Incision
Skin incision
The vascular supply to the planned flap is a dissection of the cutaneous angiosome of the lateral calcaneal (posterior peroneal) artery.
The vertical incision does not pass any more anteriorly than the Achilles tendon and, superiorly goes more posteriorly to lie in the midline to avoid damage to the sural nerve.
The horizontal incision begins at the level of the base of the fifth metatarsal bone. It is at the level of the junction of the lateral and sole skin. From the base of the 5th metatarsal it extends posteriorly strictly at the level of the lateral/inferior angle of the foot to the level posteriorly of the tip of the lateral process.
It is easiest to perform the vertical incision from superior to inferior and the horizontal incision from anterior to posterior and then join them by a gentle curve.
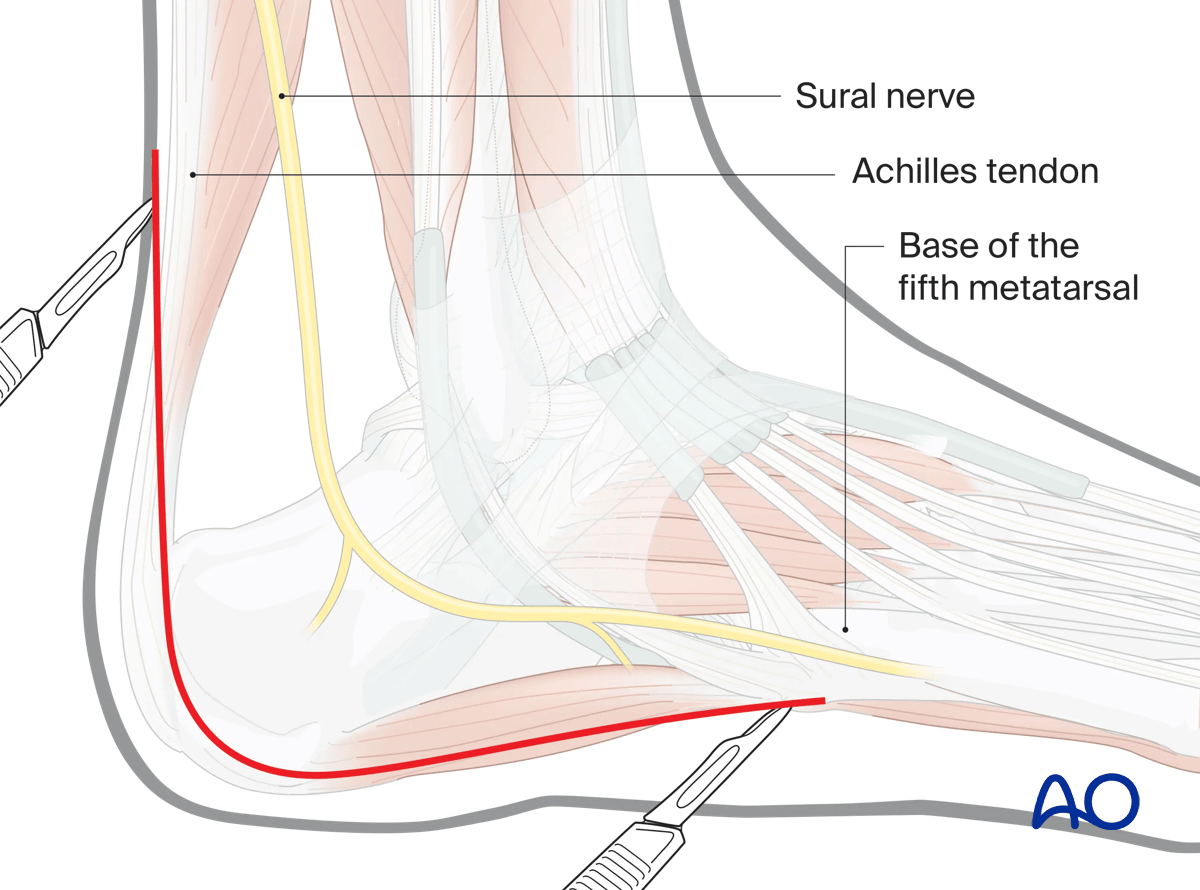
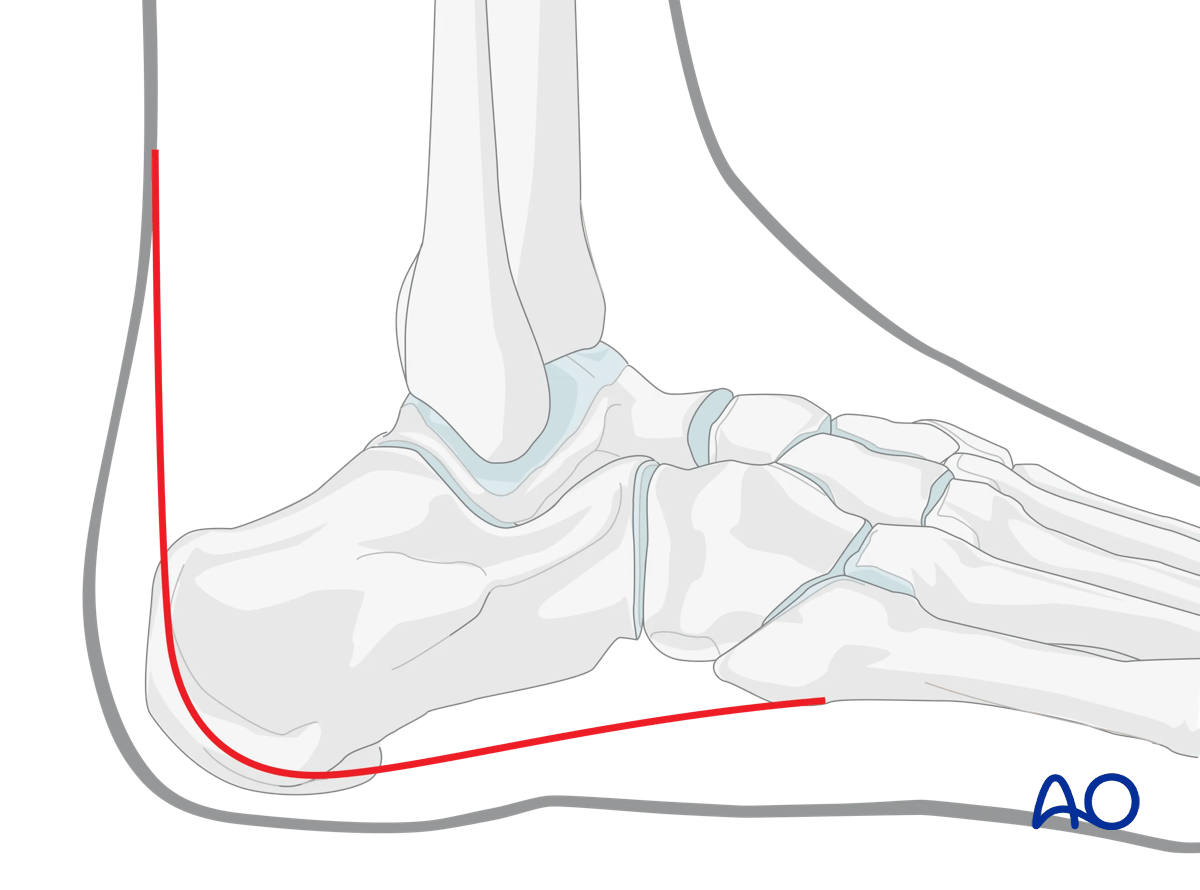
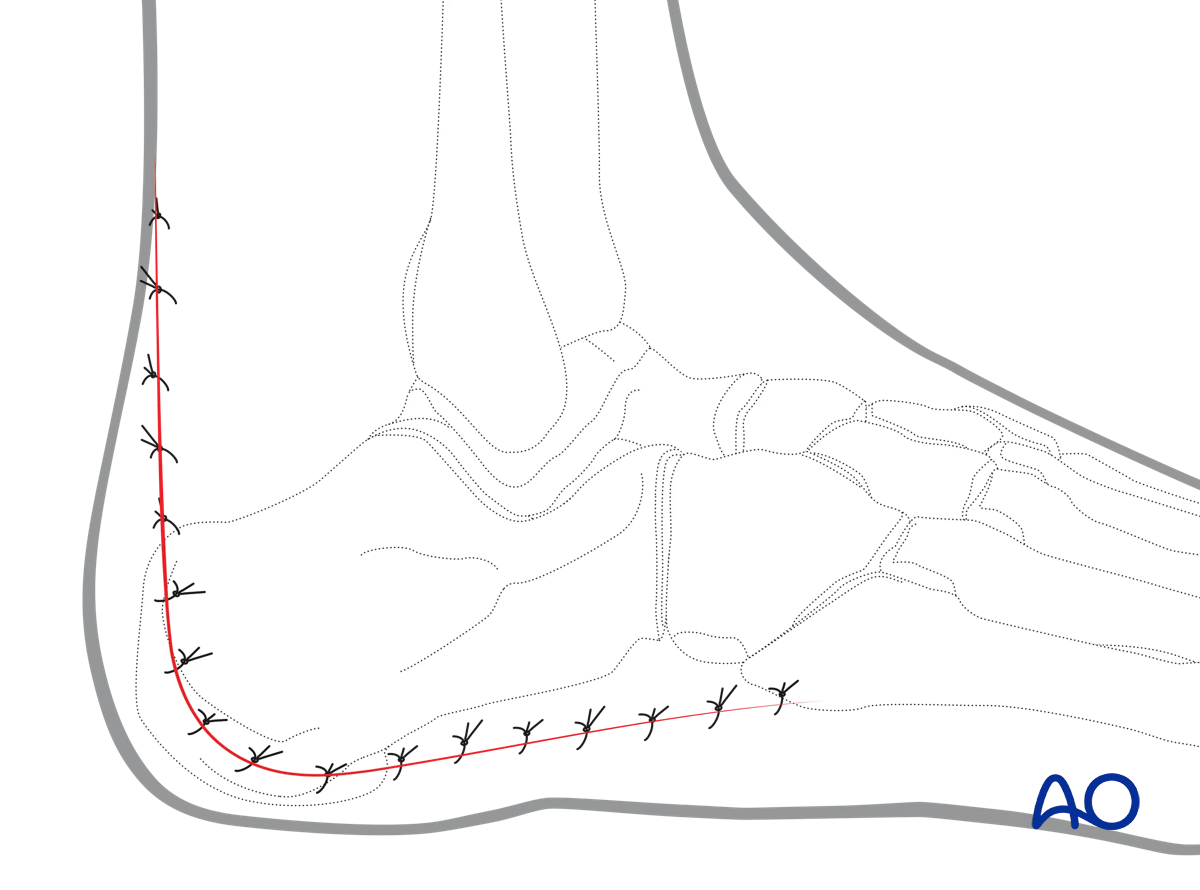
In this image, the skin incision is indicated.
Note that the horizontal part of the incision lies well below the bruising. It is at the junction of the lateral aspect of the foot and the sole.
The upper part of the vertical incision moves towards the midline to avoid the sural nerve.

Development of flap
Deep dissection commences at the junction of the vertical and horizontal limbs of the incision, cut down directly onto the inferior lateral bone of the calcaneum. Note that distally, the inferior limb of the incision is well below the calcaneum.
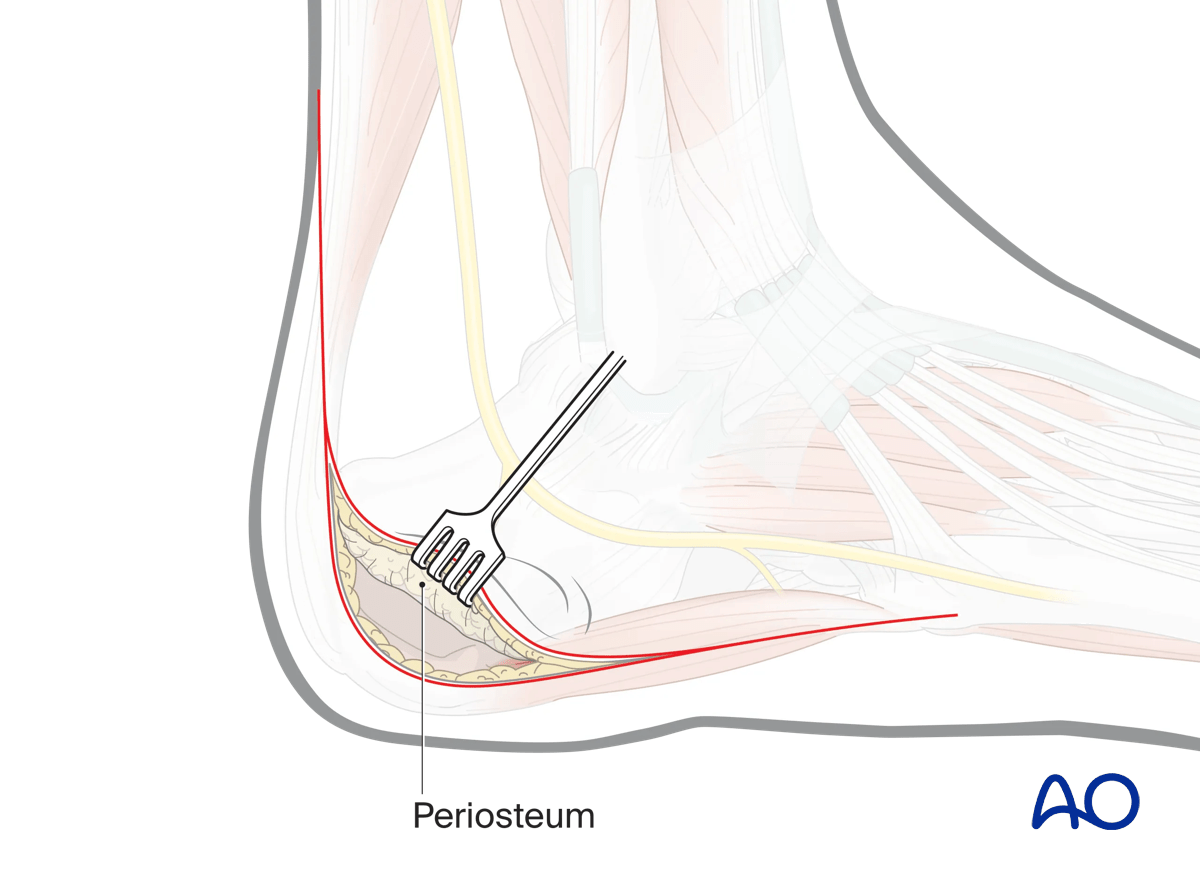
Very carefully, commence dissection maintaining a strictly subperiosteal plane, elevating the periosteum with the flap. The abductor digiti minimi brevis is split in the line of its fibers.
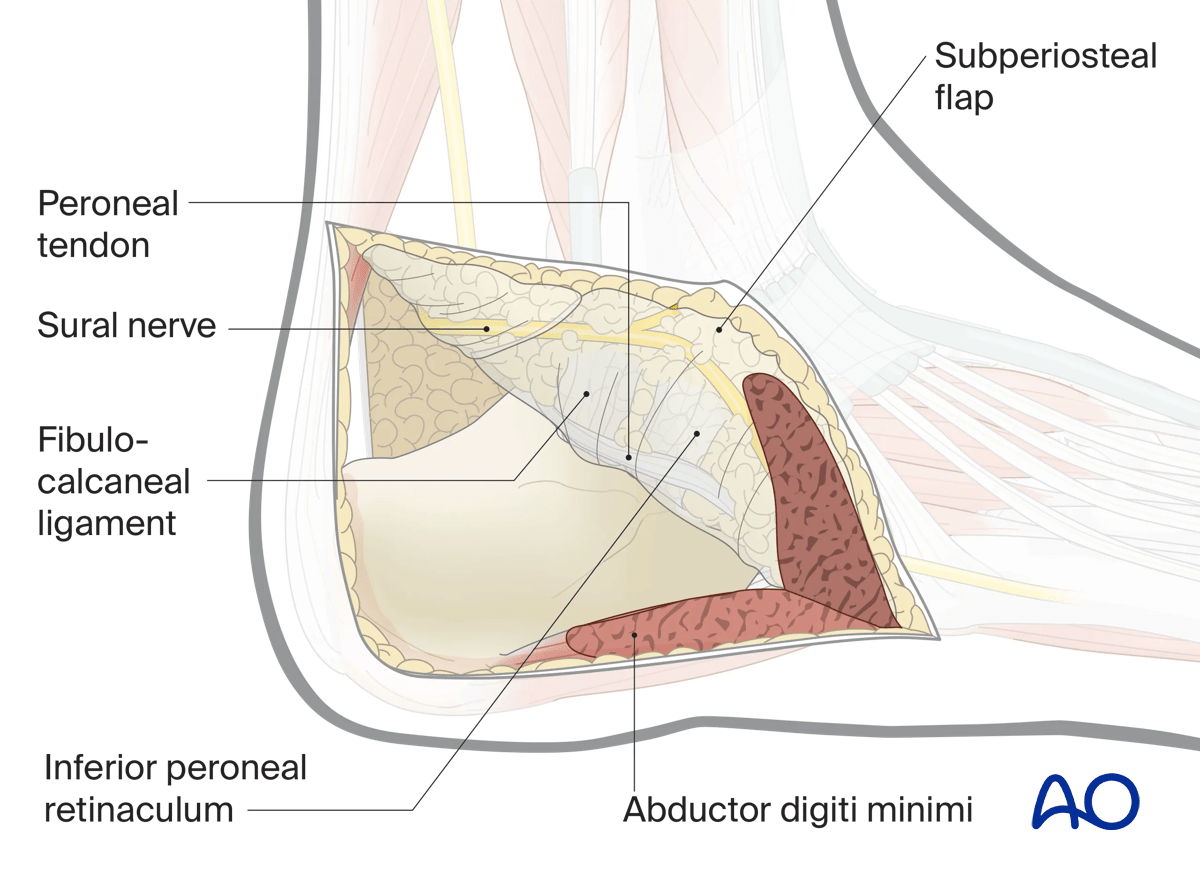
As the dissection proceeds, the lateral collateral ligament and the inferior peroneal retinaculum are elevated as one continuous layer with the periosteum.
A self-retaining retractor very carefully placed on the periosteum as it is lifted with the flap may assist dissection without endangering the flap.
Alternatively, sutures passed through the periphery of the periosteal layer may be used.
- Wu K, Wang C, Wang Q, et al. Regression analysis of controllable factors of surgical incision complications in closed calcaneal fractures. J Res Med Sci. 2014 Jun;19(6):495–501.
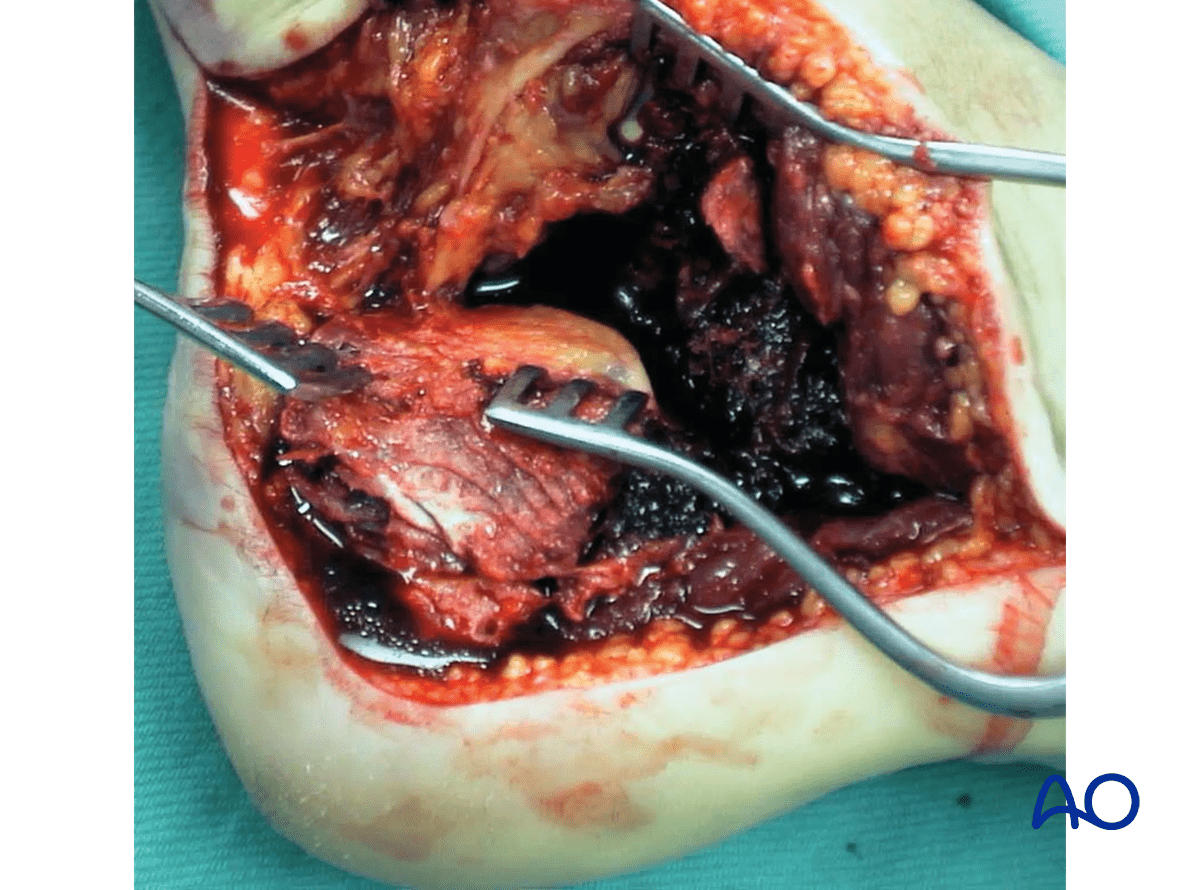
Undertaken in this way, dissection proceeds until the level of the subtalar joint, which is naturally opened as part of the dissection (solid line).
Some parts of the lateral wall may be elevated with the periosteum.
To improve exposure of the posterior facet of subtalar joint, dissection can be carried directly forward between the flexor hallucis and peroneal tendons, directly down onto the posterior aspect of the posterior facet.
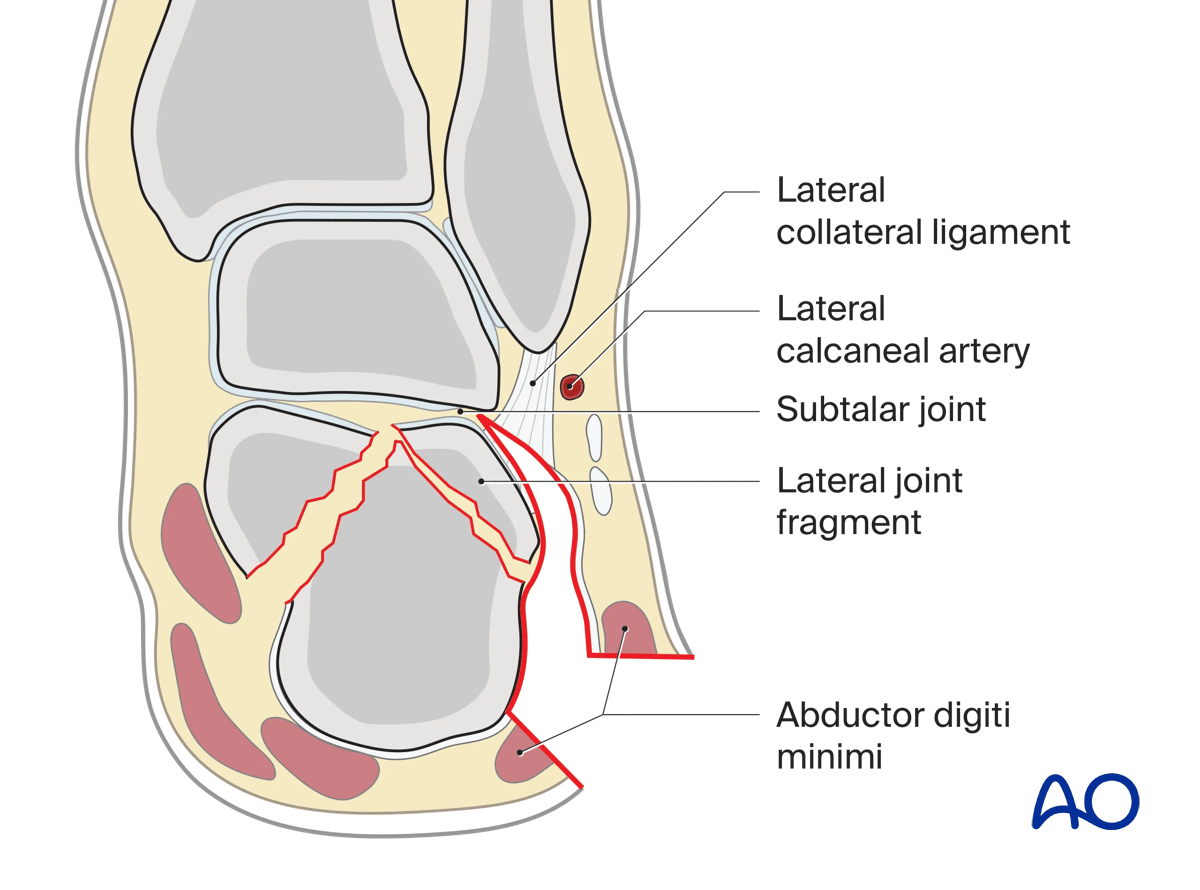
In this illustration, a semicoronal view perpendicular to the posterior facet of the subtalar joint is shown with a Sanders type-IIb/Atkins type-I fracture.
5. Wound closure
Soft-tissue closure should be carefully performed in layers. Two-level closure is standard.
The fascia over the digiti minimi is closed with an absorbable suture and posterior to the muscle the deep fascia is closed with an absorbable suture.
It may be possible to close the superficial fascia with an absorbable suture. This layer runs out in the upper end of the vertical end of the incision.
For skin closure, either a continuous subcuticular absorbable suture may be used or an interrupted suture.
A drain may be employed to decrease the risk of hematoma formation.
Healing complications
Sural nerve damage should not occur if the incision is performed correctly.
If the incision is undertaken properly, wound healing problems are rare.
In a high-energy calcaneal fracture, there may be some poor healing of the apex of the flap. It is important not to put metal work close to the apex. In these cases, the wound will heal by secondary intention with serial dressings.













