Endaural approach to the condyle
1. Principles
General considerations
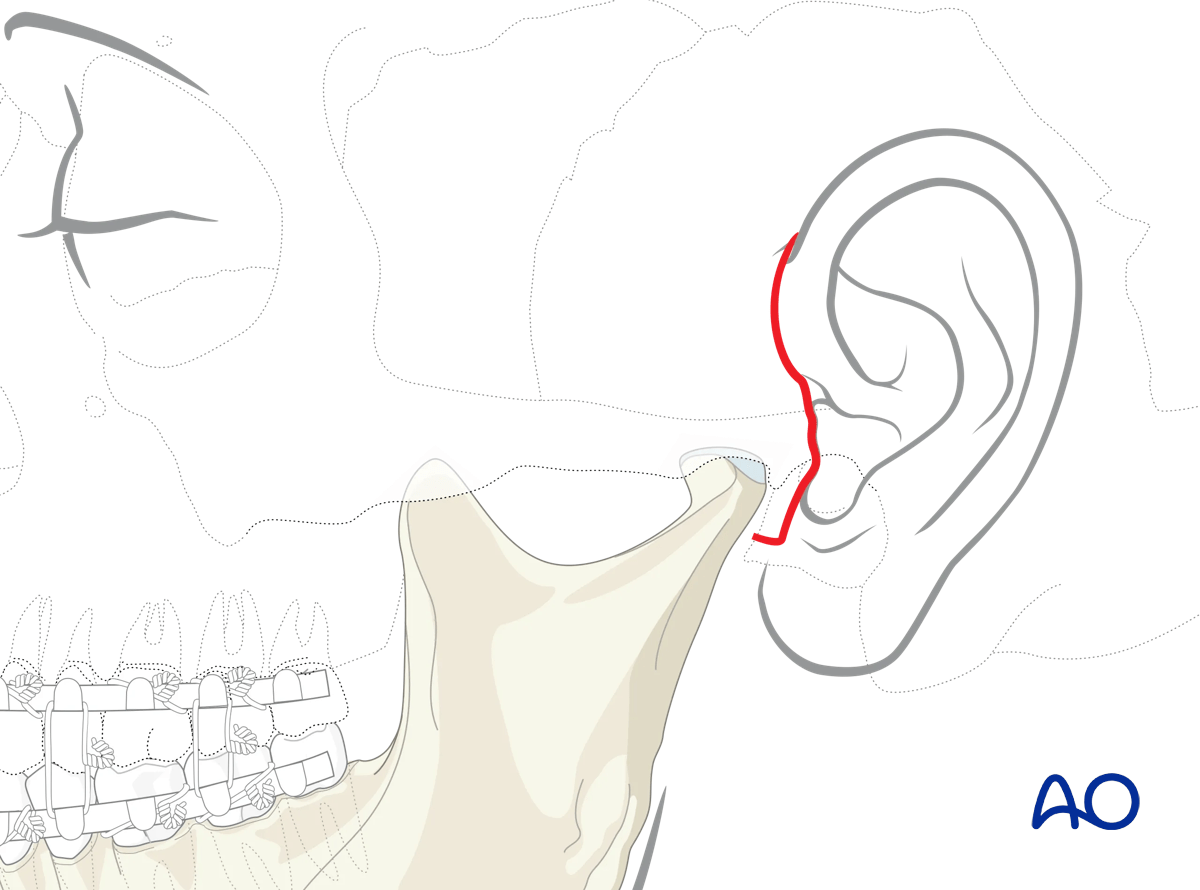
The endaural approach gives access to fractures in the mandibular condylar head and neck regions. Many surgeons who perform temporomandibular joint (TMJ) surgery routinely use this incision to access the temporomandibular joint.
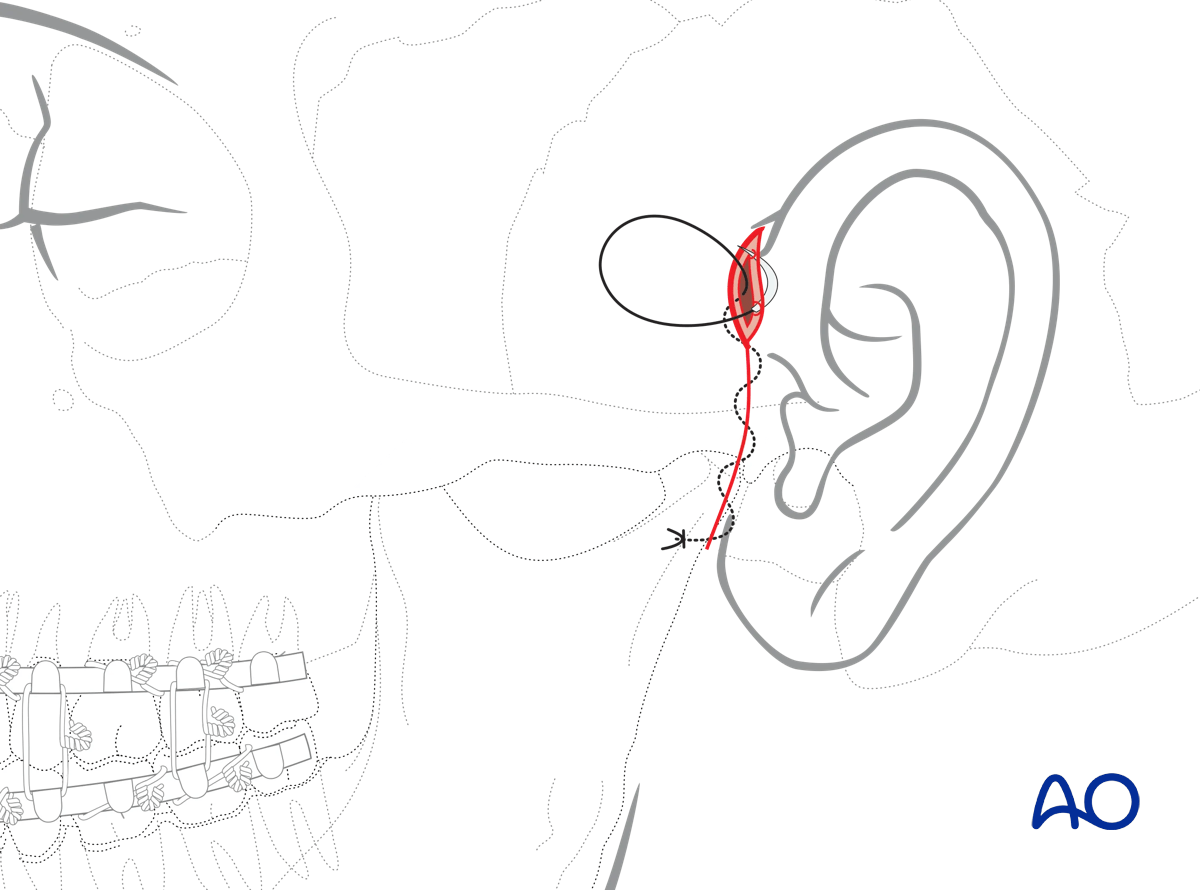
The illustration demonstrates the access and the amount of exposure.
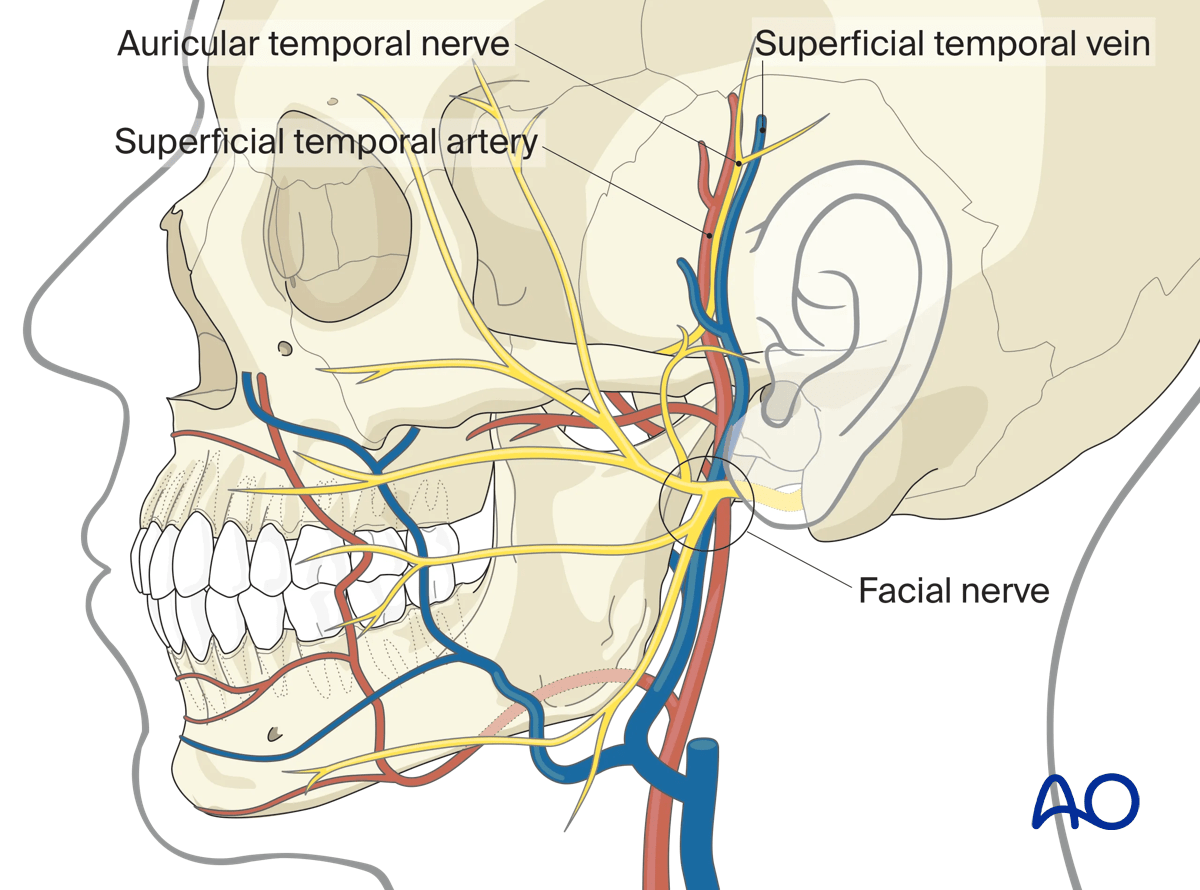
Neurovascular structures
The superficial temporal artery and vein are commonly encountered in this surgical approach. The vessels should be conserved if possible.
Branches of the facial nerve may be involved in this incision and dissection.
Exposure
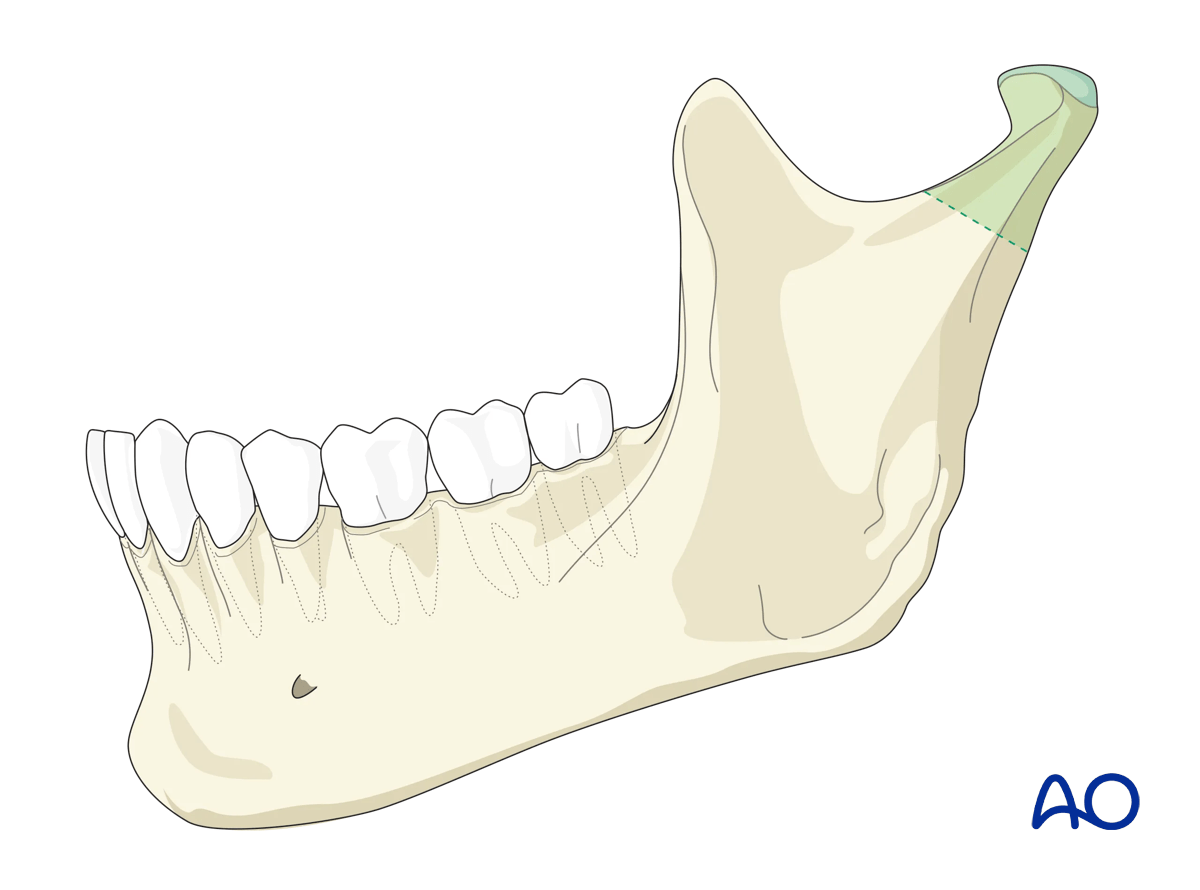
The exposure offered by the endaural approach is limited.
Only a limited portion of the condylar neck region can be reached.
2. Skin incision
General considerations
The use of a solution containing vasoconstrictors ensures hemostasis at the surgical site. The two options currently available are the use of local anesthetic or a physiologic solution with vasoconstrictor alone.
Use of a local anesthetic with vasoconstrictor may impair the facial nerve's function and impede the use of a nerve stimulator during the surgical procedure. Therefore, consideration should be given to using a physiological solution with vasoconstrictor alone or injecting the local anesthetic with vasoconstrictor very superficially.
Muscle relaxants used in general anesthesia can also impair nerve function and must be avoided.
Mark the incision in a preauricular skin crease at the superior part of the helix and extend caudally hugging the tragus to end just below the tragus.
Infiltrate local anesthetic or physiologic solution with a vasoconstrictor for hemostasis and incise the skin following the incision outline.

3. Dissection
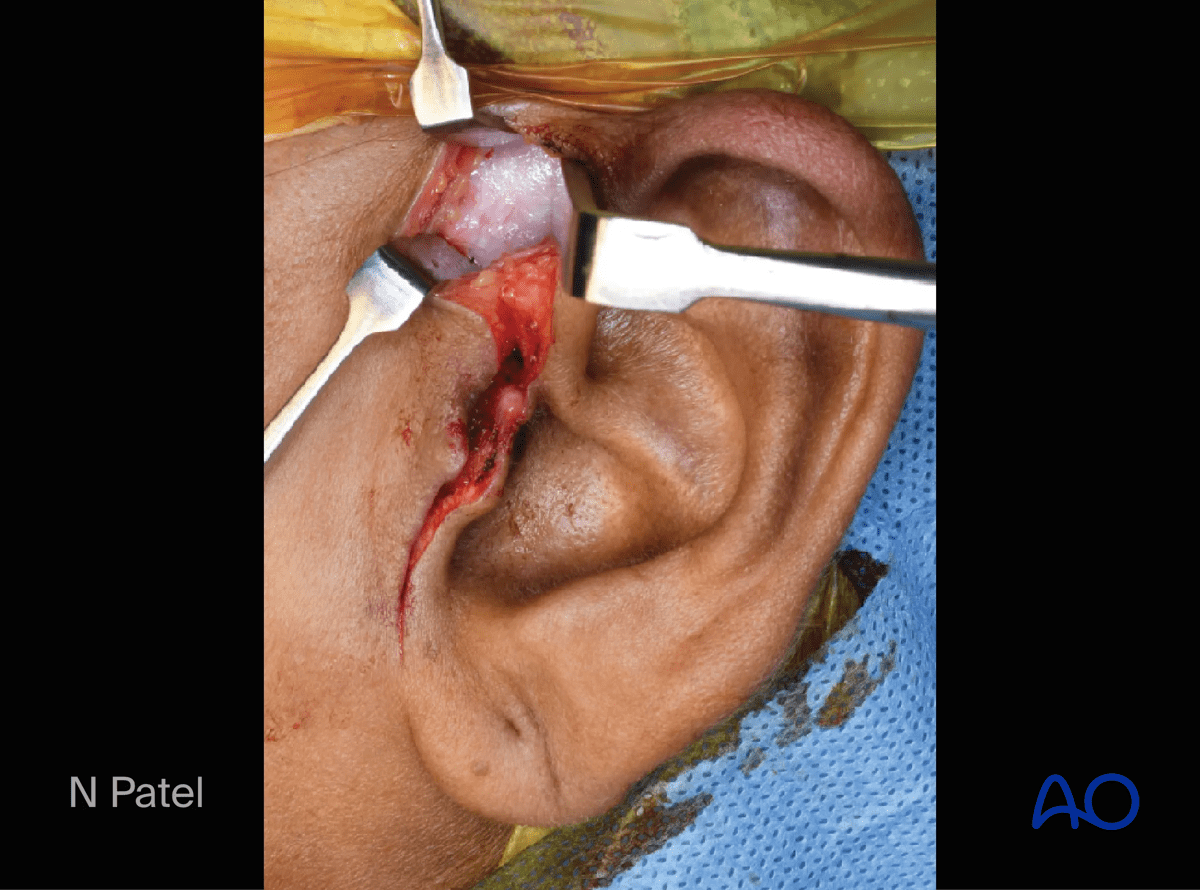
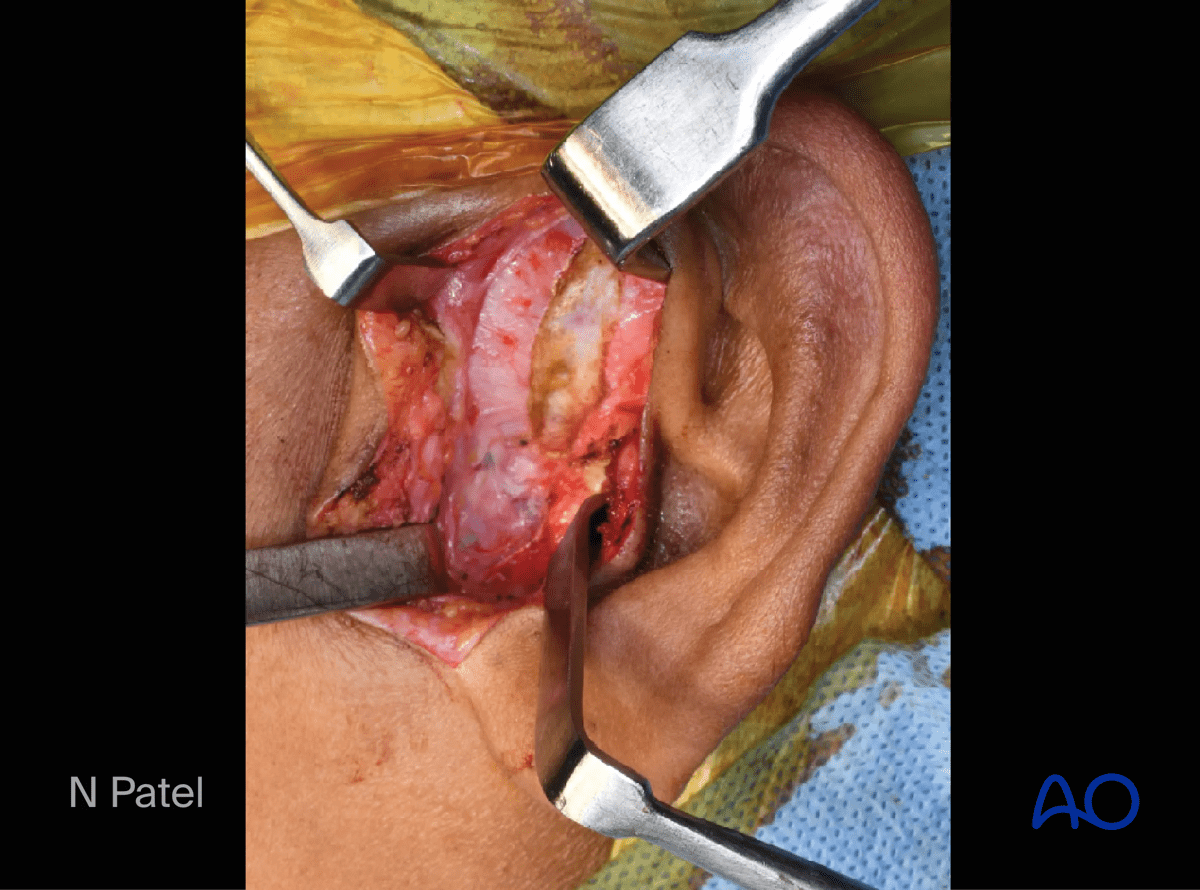
Carry the incision through the skin and subcutaneous tissue to expose the tragal cartilage at the supra-perichondrial level.
The superficial temporal vessels may be retracted anteriorly with the skin flap (sectioning some posterior and superior branches) or left in place.
The zygomatic arch can easily be palpated at this point of the dissection. The lateral pole of the mandibular condyle can also be palpated. Palpation can be facilitated by having a surgical assistant manipulate the jaw.

Locating the temporalis fascia
Continue the dissection at the cranial end to expose the deep temporal fascia.
Develop a tunnel connecting both parts of the incision.
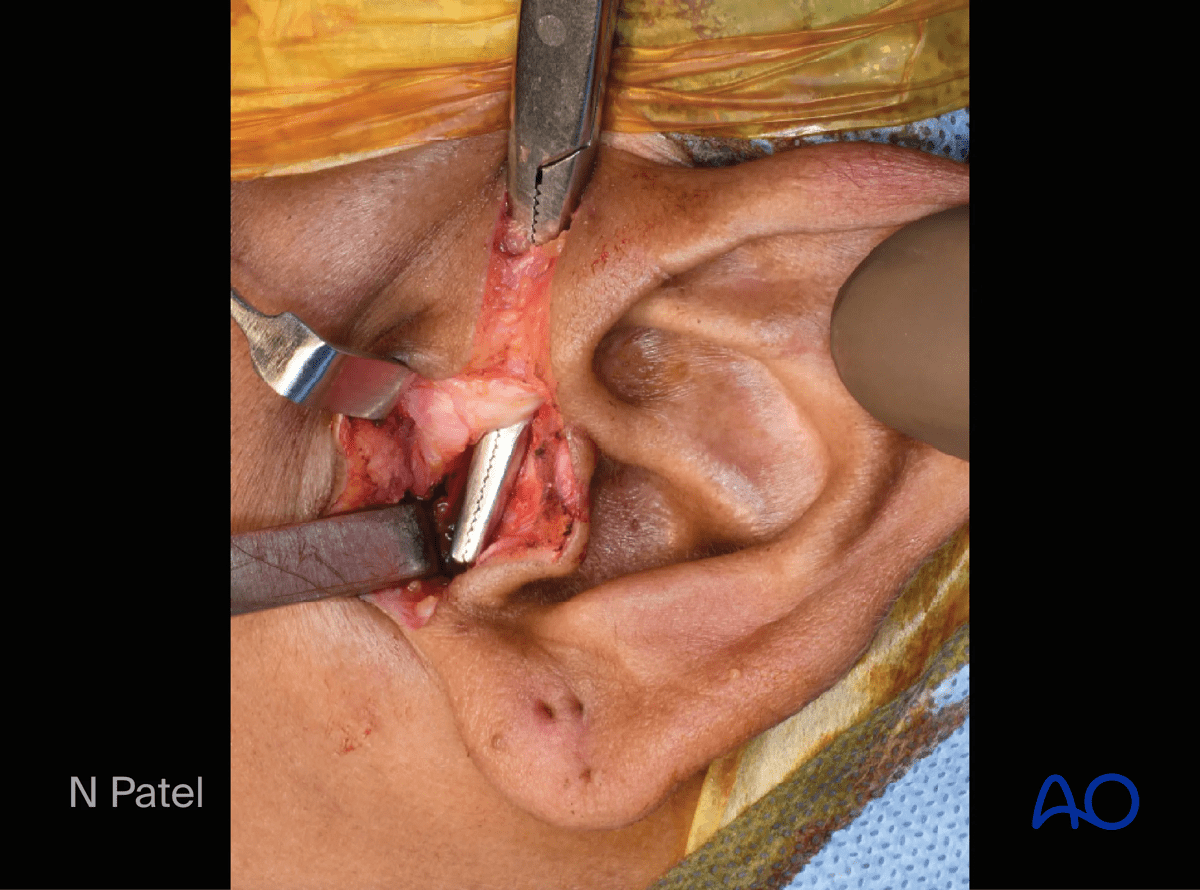
Both parts of the incisions are now connected in a single plane. Incise the overlying tissue to expose the root of the zygomatic arch.
Incising the temporalis fascia
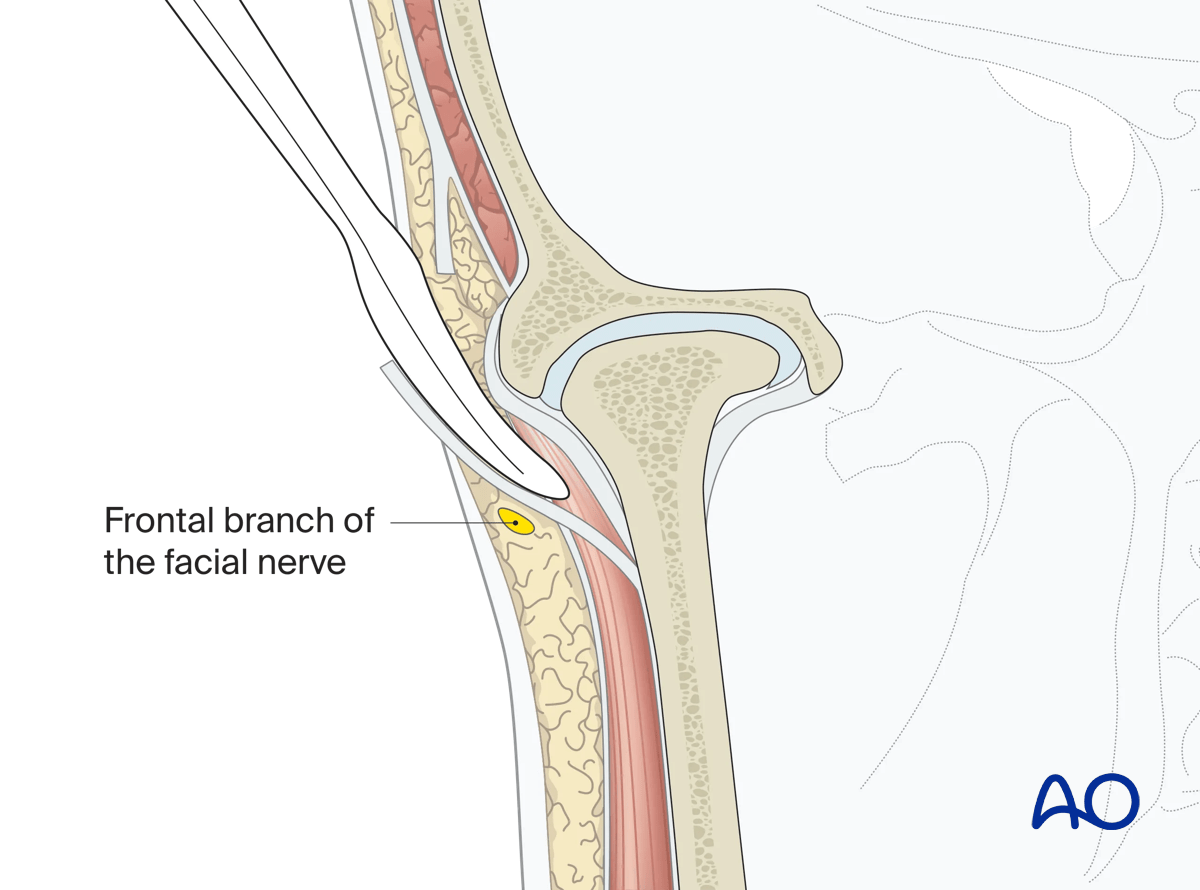
Make an oblique incision parallel to the course of the Facial nerve's frontal branch, through the superficial layer of the temporalis fascia from the root of the zygomatic arch to expose the fat plane.
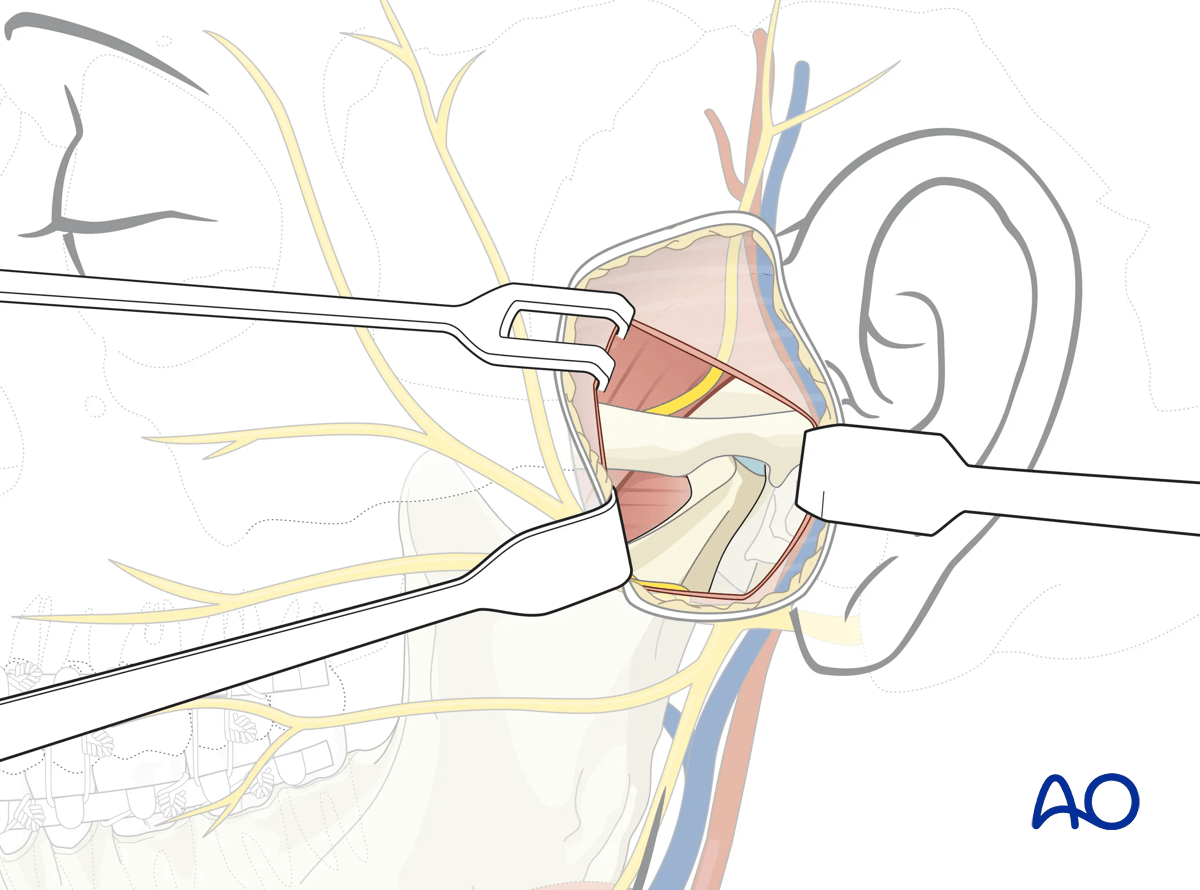
This illustration shows the coronal view of dissection to the lateral portion of the zygomatic arch and the mandibular condyle region.
Note that the facial nerve's frontal branch is protected within the superficial layer of the deep temporalis fascia.
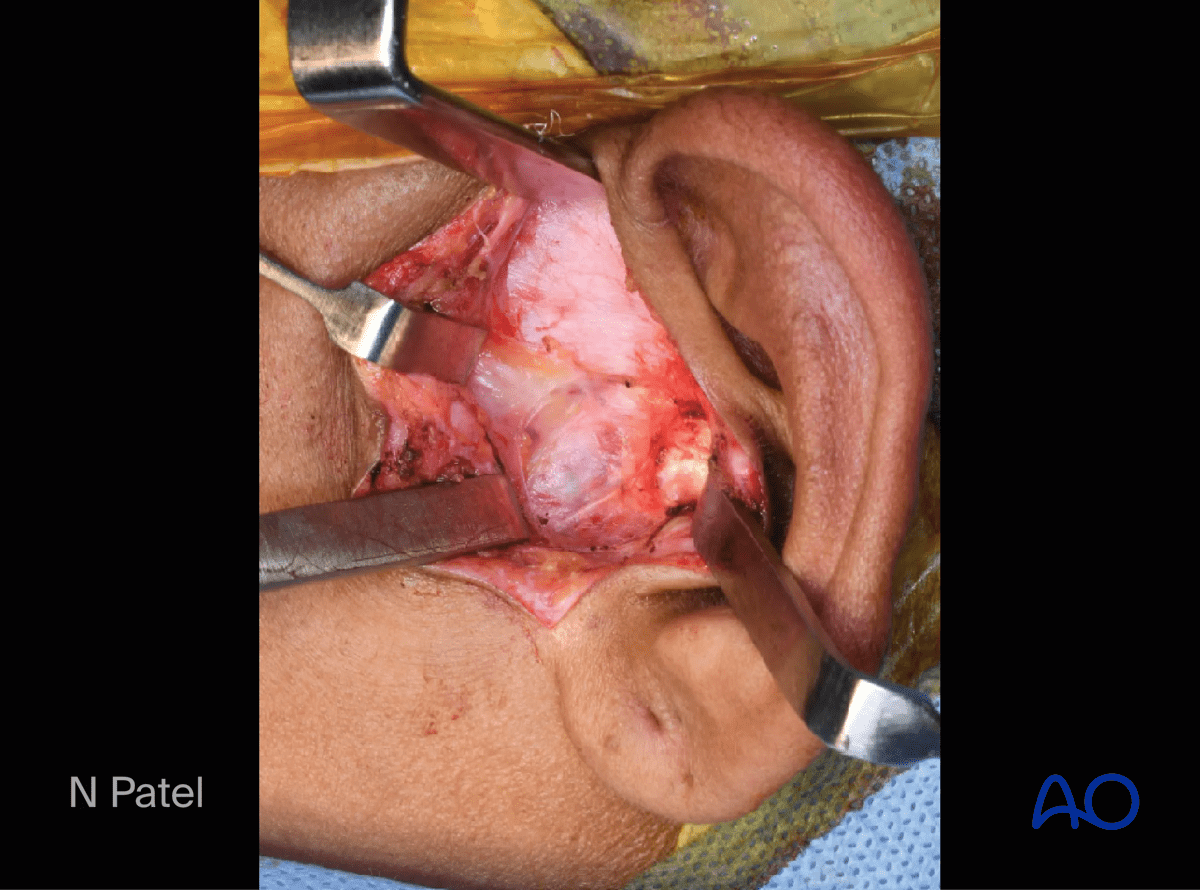
Raise the periosteum off the zygomatic arch along its length to expose both the arch and capsule of the temporomandibular joint.
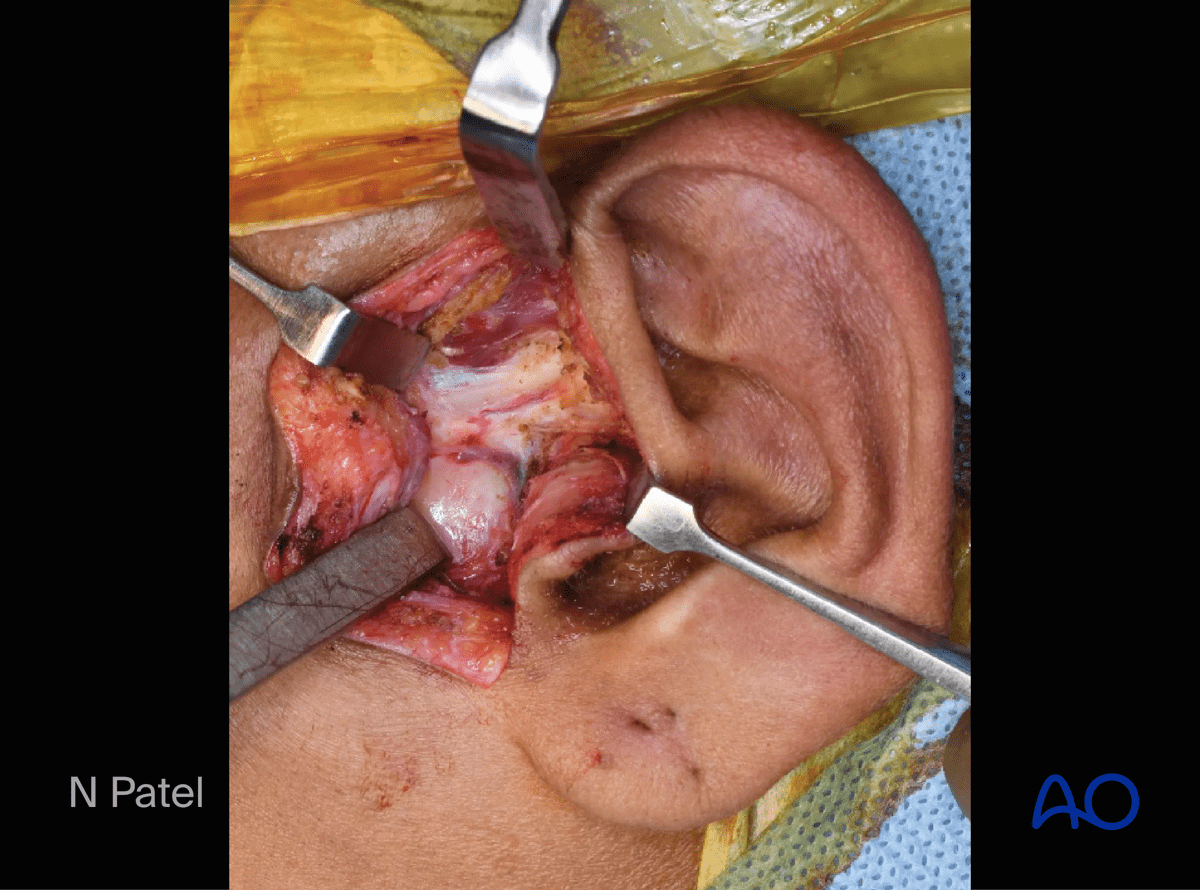
The entire zygomatic arch is exposed, revealing the articular eminence and the temporomandibular joint capsule.
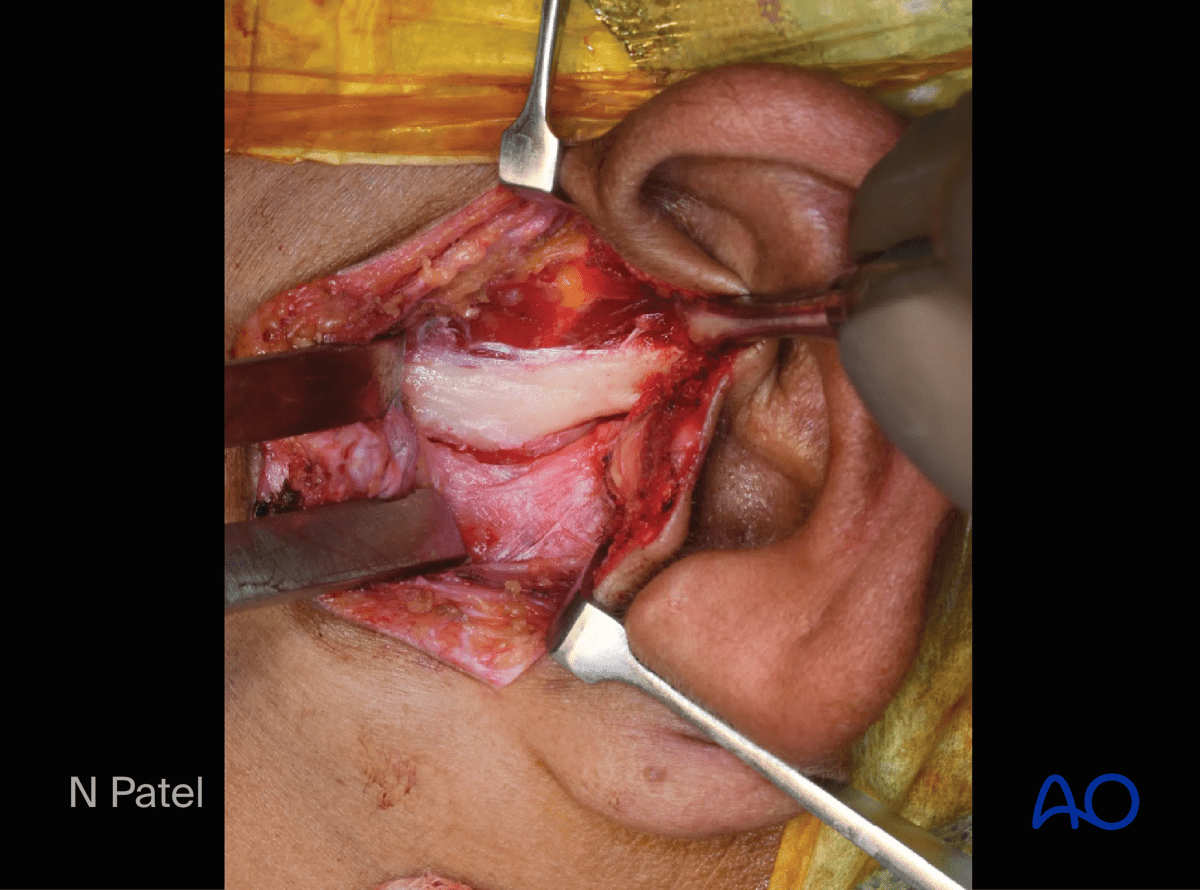
The temporomandibular joint capsule is incised horizontally to expose the condylar head.
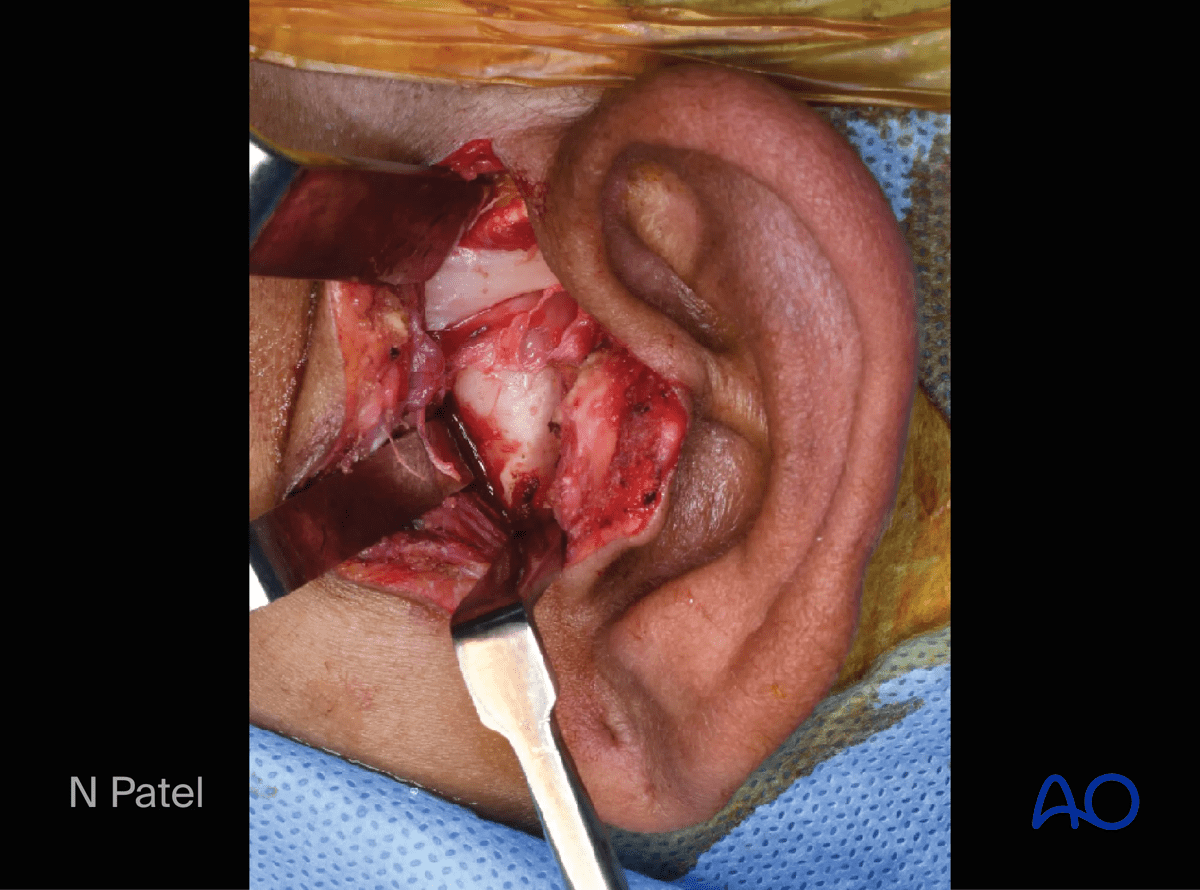
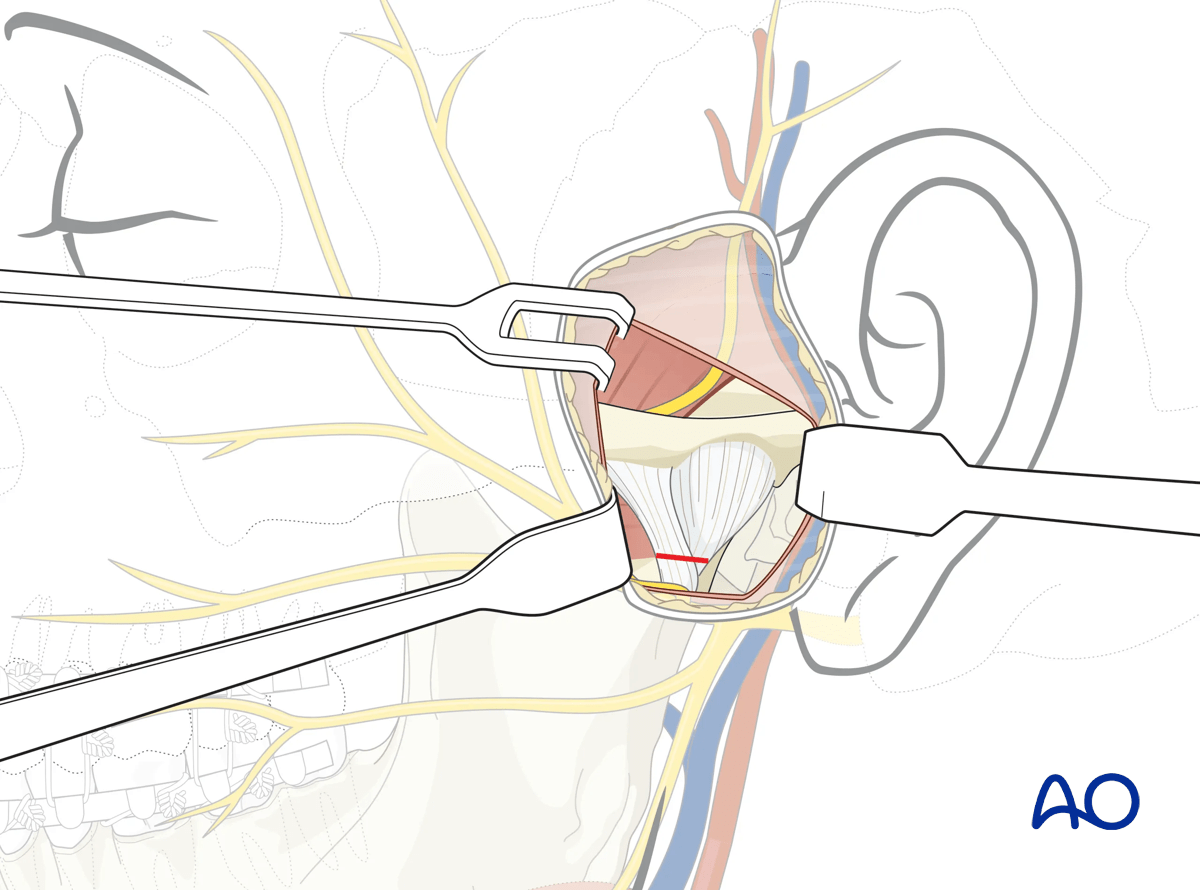
4. Optional: capsule incision
In the rare case of treating condylar head fractures, the temporomandibular joint capsule is horizontally incised at the level where the capsule meets the condylar neck.
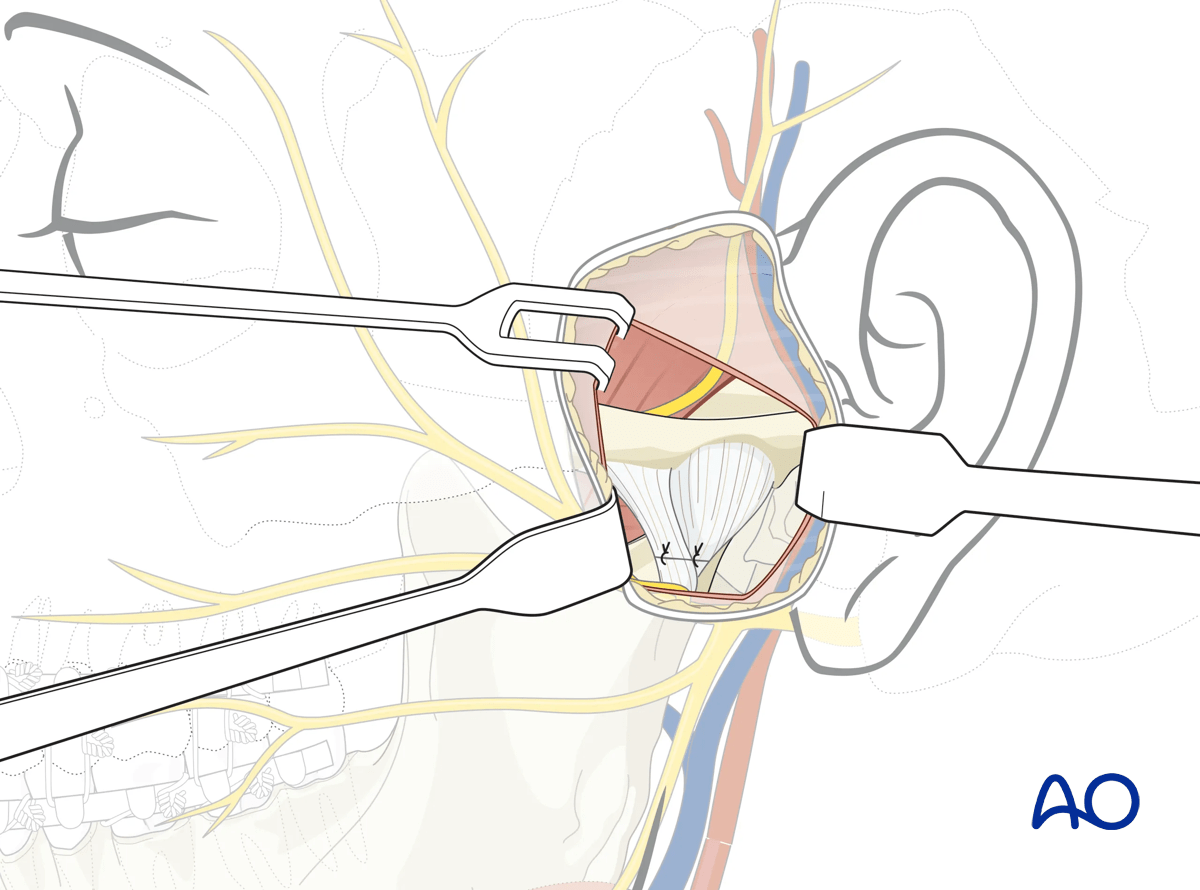
Dissection can be carried inferiorly in a subperiosteal plane to reach the neck of the mandibular condyle.
5. Wound closure
If the temporomandibular joint capsule has been incised to access the condylar head, it must be closed as the first step.
Next, the temporalis fascia is closed.
Skin and subcutaneous sutures are placed.
A pressure dressing and/or drain may be used according to the surgeon's preference.